



Original Studies
BACKGROUND: The coronavirus pandemic has had an extremely negative impact on the patients with diabetes mellitus (DM both in terms of a more severe course of COVID -19 and an increased risk of death.
AIM: Analysis of risk factors for death due to COVID -19 in patients with DM type 1 and type 2 (DM1 and DM2).
MATERIALS AND METHODS: Retrospective analysis of the database of the national diabetes register (NDR), which included DM patients with COVID-19 and reported virus infection outcome (recovery/or death) in 15 712 DM1 and 322 279 DM2 patients during a 2-year follow-up period (01/02/2020 to 03/04/2022) (discharge date)).
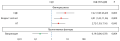
RESULTS: Case fatality rate in patients with DM, who underwent COVID -19 was 17.1% (DM1–8.8%; DM2–17.5%). As a result of multivariate regression analysis of seven significant factors in DM1 and thirteen in DM2 (evaluated by univariate anlisys), a number of the most important predictors of risk for fatal outcome were identified: in DM1 these were age ≥65 years (OR =4.01, 95% CI: 1.42–11.36), presence of arterial hypertension (AH) (OR =2.72, 95% CI: 1.03 -7.16) and diabetic foot syndrome (DFS) (OR = 7.22, 95% CI: 1.98–26.29); for T2DM: age ≥ 65 years (OR =2.53, 95% CI: 1.96–3.27), male (OR =1.51, 95% CI: 1.23–1.84), duration DM ≥10 years (OR =2.01, 95% CI: 1.61–2.51), BMI ≥ 30 kg/m2 (OR =1.26, 95% CI: 1.02–1.55), ASCVD/CKD (OR =1.49, 95% CI: 1.01–2.04), history of diabetic coma (OR =12.97, 95% CI: 1.89–88.99) and presence of disability ( OR =1.40, 95% CI: 1.14–1.73). In T2DM, the type of antidiabetic therapy (ADT) prior to COVID -19 (last visit before the development of infection) had a significant impact: Insulin therapy (OR = 1.64, 95% CI: 1.30–2.07), sulfonylureas (SU) (OR =1.51, 95% CI: 1.23–1.84)); dipeptidyl peptidase-4 inhibitor (iDPP-4) therapy (OR =0.57, 95% CI: 0.39–0.83) and sodium-glucose cotransporter-2 inhibitor (iSGLT2) therapy (OR =0.64, 95% CI: 0.46–0.88). Vaccination was the most important protective factor in both types of DM: DM1 OR =0.19, 95% CI: 0.06–0.59; SD2 OR =0.20, 95% CI: 0.16–0.26.
CONCLUSION: The common risk factor for fatal outcome in both DM1 and DM2 was age ≥65 years; in DM1 — history of hypertension and DFS, in DM2 — male sex, diabetes duration ≥10 years, BMI ≥30 kg/m2, history of ASCVD/CKD and diabetic coma, disability. In T2DM, significant differences in risk were observed depending on the type of ADT: insulin and SU therapy were factors that increased the risk of death, whereas therapy with iDPP-4 and iSGLT2 reduced the risk of death. Vaccination reduced the risk of death in DM1 and DM2 by 5.2 and 5-fold, respectively.

BACKGROUND: Russia is one of the most multinational states in the world. Identification of ethnic groups with a higher risk of developing DM2, analysis of risk factors for the development of DM2 will allow developing personalized approaches to the prevention and treatment of DM2.
AIMS: To reveal ethnic features of the prevalence of carbohydrate metabolism disorders and risk factors for the development of DM2 in the adult population of the Russian Federation.
MATERIALS AND METHODS. A retrospective analysis of the database of the national epidemiological cross-sectional study NATION was carried out. Depending on the self-specified nationality, on the basis of anthropological characteristics, the following ethnic groups were identified: “Mongoloid population”, “Peoples of the Volga region”, “Peoples of the North Caucasus”, “Peoples of Transcaucasia”, “Russians”. The analysis consisted of several stages and included: analysis of the anthropometric features of the selected groups, taking into account the presence of carbohydrate metabolism disorders (MO); study of the prevalence of violations of the MA in the selected ethnic groups; analysis of ethnic characteristics of risk factors for the development of type 2 diabetes; analysis of the frequency of violations of the MA in various ethnic groups, taking into account the territory of residence. MR disorders were defined as the presence of DM and/or prediabetes. In accordance with the WHO criteria, HbA1c≥6.5% corresponded to the diagnosis of DM, HbA1c values in the range of 5.7%≤HbA1c<6.5% to the diagnosis of prediabetes.
RESULTS: The highest frequency of violations of the MA was observed in the group «Peoples of the Volga region» (31.2%), the lowest in the «Peoples of the North Caucasus» (15.6%). BMI in the group “Peoples of the Volga region” was significantly lower than in the group “Peoples of the North Caucasus. Violations of MR were more often observed in the abdominal nature of obesity, obesity of the 1st stage, age over 45 years in the groups «Mongoloid population» and «Peoples of the Volga region» than in the peoples of the «Northern Caucasus» and «Transcaucasia». The frequency of occurrence of SR violations among representatives of the Volga Peoples group living in their historical territories was higher than among Russians living in the same regions: 32.5% and 24.3% (p<0.001 χ2 criterion), and also higher than in the Russian CFD: 32.5% and 27.4%, respectively, p=0.001 (χ2 test). The prevalence of violations of the MA among the peoples of the North Caucasus was less than among the Russians of the Central Federal District — 13.9% and 27.36%, respectively (p<0.001 χ2 criterion). The prevalence of MR violations among representatives of the “Peoples of the North Caucasus” group living in their historical territories (n=598) was less than among those living in other regions of the Russian Federation (n=164) (13.9% and 21.95%, p= 0.012 criterion χ2).
CONCLUSION: In the present work, for the first time, we analyzed the prevalence of MR disorders in various ethnic groups of the population of the Russian Federation, identified certain ethnic characteristics of DM2 risk factors and their contribution to the development of the disease. The obtained results should be used for planning preventive programs in various regions of the Russian Federation.
BACKGROUND: The widespread use in clinical practice of drugs with cardio- and nephroprotective properties, in particular, sodium-glucose cotransporter type 2 inhibitors (SGLT2i), is based on the results of large-scale international randomized trials. Meanwhile, there are no data demonstrating the possibility of the influence of these drugs on mortality rates in real clinical practice in Russian patients. To study this issue, a CARDIA-MOS study was conducted on a population of patients with type 2 diabetes (T2DM) in Moscow.
AIM: To study the effect of SGLT2i on the total mortality of patients with T2DM in Moscow.
MATERIALS AND METHODS: To assess the frequency of different outcomes, two samples of patients were formed according to predetermined criteria: 1) patients who started therapy with SGLT2i (dapagliflozin) in 2017; 2) a control group of patients corresponding to the main group in terms of key indicators: age, duration of T2DM, presence of cardiovascular diseases, use of insulin therapy, HbA1c level.
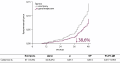
RESULTS: Firstly, an analysis of the data of 499 patients who started treatment with dapagliflozin in 2017, as well as 499 patients in the control group (n = 998) was made. The baseline characteristics of the patients were generally comparable. Pre-study SBP and HbA1c were worse in the dapagliflozin group. The use of dapagliflozin was associated with a 39% reduction in the relative risk of death from all causes (RR 0.614, 95% CI 0.417–0.903, p = 0.013), led to a decrease in HbA1c levels by 0.8% (from 8.5 to 7.7%, p<0.001) for 48 months. observations. The safety profile of dapagliflozin was comparable to that of the control group
CONCLUSION: The use of dapagliflozin in the treatment of patients with T2DM can reduce overall mortality and improve glycemic control.
BACKGROUND: T1D is characterized by autoimmune destruction of pancreatic β-cells, which develops due to genetic and environmental risk factors. Shortly after initiating the treatment with insulin, 80% of children with T1D may require smaller doses of insulin and develop clinical and laboratory remission of the disease so called «honeymoon». The issue of whether there is a need of differential diagnosis between autoimmune DM and non-immune forms of DM raises in cases of preclinical diagnosis of T1D and laboratory remission for more than 6 months.
AIM: To study the clinical, immunological, genetic characteristics of T1D remission phase and MODY in children, to determine the diagnostic criteria for T1D and MODY in children.
MATERIALS AND METHODS: A single-centre, cross sectional noncontrolled comparative study of two independent cohorts. Data of 150 children examined in the Endocrinology Research Center (January 2016–June 2021). First cohort included patients with complete clinical and laboratory remission of T1D (n=36), second cohort included patients with MODY, confirmed by genetic study (n=114).
RESULTS: The median age of diabetes manifestation was significantly higher in patients with T1D — 11.25 years [8.33; 13.78] than in patients with MODY — 7.5 years [4.6; 12.2] (p=0.004). In patients with T1D remission the level of glycated hemoglobin was 6.0% [5.6; 6.4], in group with MODY — 6.5% [6.2; 6.7] (p<0.001). Patients with monogenic diabetes had impaired fasting glucose — 6.27 mmol/l [5.38; 6.72], while patients with remission phase had normoglycemia — 5.12 mmol/l [4.17; 5.87]. The oral glucose tolerance test was perform to all patients, two-hour glucose level did not significantly differ in two groups (p=0.08). A strong family history of diabetes in patients with MODY registered more often (93% vs. 66.7%). A positive autoantibody titer detected more often in patients with remission of T1D (77.8%) than in patients with MODY (11.4%). In addition, no more than 1 type of autoantibodies was detected in patients with MODY.
CONCLUSION: Antibodies ZnT8 and IA2 showed the greatest significance for the differential diagnosis of T1D and MODY in cases with long absents of insulin requirement in children with diabetes mellitus. Genetic test is recommended in seronegative cases. If only one type of AT is detected, specialist should decide on the need to do diagnostic genetic test based on a comprehensive analysis of the patient’s clinic characteristics, including family history, manifestation and blood glucose levels.

BACKGROUND: Postprandial hyperglycaemia contributes significantly to the lack of glycaemic control in patients with type 1 diabetes mellitus (DM1). At least a quarter of patients forget to inject insulin before meals once a week, and more than 40% of them inject bolus insulin immediately before meals, which does not correspond to the pharmacokinetic effects of ultrashort insulins and determines the need to use insulins with better imitations of physiological insulin secretion.
AIM: To assess the effect of fast acting insulin aspart (FIAsp) on the current parameters of glycaemic control in children with DM1 after switching from insulin Asp (iAsp) using continuous glucose monitoring.
MATERIALS AND METHODS: A multicenter observational 12-week prospective open-label uncontrolled comparative study was initiated. A group of insufficiently controlled patients were identified (n = 48) including a group on multiple insulin injections therapy (MII) (insulin degludec and IAsp) and a group on continuous subcutaneous insulin infusion (CSII) of iAsp. Three 14-day flash glucose monitoring (FMG) were performed: before transferring patients to FiAsp and after 2 and 12 weeks of the transfer. Key endpoints: HbA1c after 2 and 12 weeks on FiAsp relative to baseline, analysis of 5 FMG target glucose ranges, presented as an ambulatory glycemic profile. Additional indicators: dynamics of insulin daily dose, frequency of glucose self- monitoring, the number of severe hypoglycemia, adverse events that occurred during treatment.
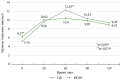
RESULTS: 2 weeks after the transfer from IAsp to FIAsp, TIR increased in the entire group of patients: from 53% [44.3; 66.5] to 57% [47.4; 71.0] (p-value = 0.010) and TAR decreased from 38% [24.8; 50.2] to 30.5% [22.0; 45, 0] (p-value = 0.0124). Maintaining and increase time spent in the target glucose ranges during a 12-week observation period, in parallel with a significant decrease in hypoglycemic episodes <3.9 mmol / L per week, on FIAsp therapy naturally leads to an improvement in diabetes control: a decrease in HbA1c from 8.15% up to 7.75% (p-value = 0.0224), more pronounced in the group of patients on CSII — from 7.9% to 7.5% (p-value = 0.028).
CONCLUSION: Switching from IAsp to BDIAsp in routine clinical practice in the MII and CSII regimen in children and adolescents with type 1 diabetes allows achieving better glycemic control compared to the previous generation prandial insulin analog Iasp. The better diabetes control is associated with an increase or a trend towards an increase in TIR and a decrease or a trend towards a decrease in TAR and TBR, as well as a significant decrease in episodes of hypoglycemia.

BACKGROUND: Diabetes mellitus (DM) is a predisposing factor for the development of many infectious complications. Numerous studies have demonstrated the association of hyperglycemia in patients having DM with a high risk of a more unfavorable course of COVID-19. However, hyperglycemia is often detected in patients with a COVID-19 not having anamnesis of DM. The following remains unclear: the etiological factors causing such disorders of carbohydrate metabolism, the persistence of these disorders and the characteristics of the course, as well as their comparative effect on the outcomes of COVID-19 and the further prognosis of patients.
AIM: To study the prevalence and nature of carbohydrate metabolism disorders in patients with moderate to severe course of COVID-19, as well as 6 months after it.
MATERIALS AND METHODS: Hospitalized patients with a confirmed diagnosis of COVID-19 of moderate and severe course of the disease were examined. There were no medical interventions outside recommendations of patient management. The observation was carried out during two time periods: inpatient treatment of a COVID-19 and 6 months after discharge. The following were evaluated: anamnesis data, the level of fasting plasma glucose; HbA1c, the results of computed tomography of the lungs, the drug therapy taken in all patients. Descriptive statistics methods were used to evaluate the parameters.
RESULTS: The study included 280 patients with a median age of 61.5±14,2 years. During the disease, a violation of carbohydrate metabolism was detected in 188 people (67%), the remaining patients (33%) made up the normoglycemia group. Patients with hyperglycemia were stratified in a following way: a group with an established diagnosis of DM before COVID -19 included — 56 people (20%), a group with steroid-induced hyperglycemia (SIH) — 95 people (34%), a group of stress- induced hyperglycaemia — 20 people (7%), with undiagnosed diabetes — 17 people (6%). In the postcovid period (after 6 months), the normal level of glycemia in the same sample group was observed in 199 people (71.4%); 8 people (3%) were diagnosed with new cases of DM. The mortality rate was 10 people (3.6%) in the group of SIH (8 people) and undiagnosed DM (2 people).
CONCLUSION: The use of glucocorticoids in hospitalized patients with COVID-19 leads to high incidence of SIH, which has reversible character. About 6% among hospitalized patients with a COVID-19 had undiagnosed DM and were not receiving antihyperglycemic therapy. The highest mortality was noted in the group of SIH, which allows us to conclude that SIH worsens the prognosis of patients to the greatest extent. Patients with newly diagnosed hyperglycemia, regardless of the level of hyperglycemia, are characterized by a more unfavorable course.
BACKGROUND: A decrease in the frequency of amputations due to diabetic foot syndrome (DFS) is one of the parameters that determine the quality of medical care for patients with diabetes mellitus.
AIM: Our aim was to study the indicators characterizing medical care for patients with lower limb pathology in diabetes mellitus in St. Petersburg from 2010 to 2021.
MATERIALS AND METHODS: Annual reports on the treatment of patients with DFS in city hospitals specializing in the surgical treatment of DFS and in outpatient offices «Diabetic foot» (DFO) from 2010 to 2021 were analyzed.
RESULTS: The average number of patients per year admitted to the DFO was 18,527 (34,440 visits). Proportion of patients with foot ulcers — 8,9%, with Charcot’s arthropathy — less than 1%. Before 2020, the frequency of above the foot amputations decreased from 48.3% to 8.6%, hospital mortality — from 11.7 to 5.7%, the number of revascularizations increased from 37 to 642 per year. The increase in operational activity was not accompanied by a decrease in the frequency of amputations (59.3% in 2019). Of all amputations, 11.3% were patients referred from DFO. During the epidemic, the number of visits and patients admitted to the DFO decreased by 27,3% and 31%, respectively. The proportion of foot ulcers and the frequency of amputations have not changed. Inpatient care was characterized by a decrease in operational activity, a decrease in the availability of revascularization, a 2-fold increase in the proportion of high amputations and an increase in hospital mortality from 5.7% in 2019 to 14.9% in 2021.
CONCLUSION: An analysis of the statistics of specialized care for patients with DFS over 12 years showed the reduction of the frequency of high amputations, but revealed an increase in the frequency of surgical interventions in DFS against the background of an almost unchanged proportion of amputations in the structure of all operations. Despite significant quantitative indicators, the outpatient service seems to be insufficiently effective in reaching the target population. The negative impact of the epidemic has led to a significant increase in the frequency of high amputations and mortality.
BACKGROUND: Diabetic neuroosteoarthropathy (DNOAP, Charcot foot) is a relatively rare complication of diabetes mellitus (DM), which can lead not only to impaired support function of the lower limb in such patients, but also to high amputation. DNOAP is characterized by persistent aseptic inflammation of the bone structures of the foot, which creates significant difficulties in planning therapeutic measures. In the medical literature, there are data demonstrating the role of individual cytokines and neurohumoral factors in the prolongation of the inflammatory process in diabetes, however, there are currently very few studies that determine reliable markers of aseptic inflammation in DNOAP.
AIM: To study the effect of neurohumoral factors and advanced glycation end products on the activity of aseptic inflammation in the bone structures of the foot in patients with type 2 diabetes mellitus (DM2) and diabetic neuroosteoarthropathy.
MATERIALS AND METHODS. The study included 88 patients with type 2 diabetes (45 men, 43 women). Group 1 consisted of patients with DM2 and inactive DNOAP (n= 43), group 2 (n= 45) consisted of patients with DM2 and distal diabetic neuropathy without osteoarticular pathology. The diagnosis of diabetic neuropathy was based on the analysis of the clinical picture and indicators of peripheral sensitivity. Diagnosis of DNOAP and determination of its stage was based on clinical data, the results of infrared thermometry and radiology tests of the foot bones. General clinical assessment was used, radiology tests (X-ray, MRI), evaluation of CRP, calprotectin, copeptin, glutathione peroxidase 1 (GP1).
RESULTS. According to the results of examination and palpation of the feet, as well as the analysis of the temperature gradient of the skin of the affected and contralateral limb (infrared thermometry), DNOAP was detected and the stage of this complication was determined. The diagnosis of the chronic stage of DNOAP was confirmed by the results of MRI and the clinical picture (no difference in skin temperature on the symmetrical areas of the feet). According to the results of laboratory analysis, a statistically significant difference in copeptin values was revealed — in group 1 — 0.232 µg/ml [0.147; 0.342], in group 2 — 0.115 µg/ml [0.065; 0.203] (p>0.05) and CRP — in group 1 — 7.113 mg/l [2.453; 16.505], in group 2 — 2.187 mg/l [1.131; 5.567] (p>0.05), leukocyte levels in the groups did not differ significantly: group 1 — 7.86 [6.40; 9.00]*10^9, group 2 — 7.00 [6.00; 8.15] (p>0.05). There was a trend towards an increase in the level of calprotectin and glutathione peroxidase-1 in the DNOAP group, however, the differences were not significant. calprotectin — in group 1 — 1.948 [1.229; 2.969], in group 2 — 1.692 [1.16; 2.514] μg/ml and glutathione peroxidase-1 in group 1 — 24.72 [20.1; 31.82], in group 2 — 22.98 [18.94; 31.2] ng/ml.
CONCLUSION. In the study, statistically significant differences were obtained in the levels of copeptin and C-reactive protein: in patients with DNOAP, their values were significantly higher, which indicates the persistence of the aseptic inflammatory process in the bone tissue of patients even in the chronic stage of DNOAP. These data may help in deciding whether to use one or another method of unloading the affected joints, which will affect the clinical prognosis. The study of neurohumoral markers of arthropathy in the blood serum of patients with DM2 is carried out for the first time, and therefore it is difficult to compare with the results of other authors. It can be assumed that copeptin and CRP are significant markers of persistent inflammation of the osteoarticular structures of the foot in DNOAP.
BACKGROUND: Widespread clinical use of drugs with cardioprotective/nephroprotective properties – particularly sodium-glucose cotransporter type 2 inhibitors (SGLT2i) – is based on results of large-scale international randomised trials. Meanwhile, there are no data demonstrating a potential effect of these drugs on mortality rates in real clinical practice in Russian patients. To address this lacuna, CARDIA-MOS study was conducted on a population of patients with type 2 diabetes (T2D) in Moscow.
OBJECTIVE: To study the effect of SGLT2i on total mortality in T2D patients in Moscow.
MATERIALS AND METHODS: To evaluate the frequency of different outcomes, two samples of patients were selected according to predetermined criteria: 1) patients who started SGLT2i (dapagliflozin) therapy in 2017; 2) a control group (no SGLT2i administration) matching the dapagliflozin group in terms of key indicators: age, T2D duration, cardiovascular diseases, insulin therapy, HbA1c level.
RESULTS: At Phase 1, data of 499 patients who started dapagliflozin treatment in 2017 were analysed against those of the 499 control group patients (n=998). The groups’ baseline characteristics were generally comparable. Pre-study SBP and HbA1c were worse in the dapagliflozin group. The use of dapagliflozin was associated with a 39% reduction in the relative risk of death from all causes (RR 0.614, 95% CI 0.417–0.903, p=0.013), led to a decrease in HbA1c levels by 0.8% (from 8.5 to 7.7%, p<0.001) over the 48-month-long observation.
CONCLUSION: The use of dapagliflozin in the treatment of T2D patients can reduce overall mortality and improve glycaemic control.
Review

Diabetes mellitus type 2 (DM2) is socially important disease, becoming non-infectious epidemic due to increasing prevalence. Chronic kidney disease (CKD) is one of the most common diabetic complications. Kidney injury signs and/or estimated glomerular filtration rate (eGFR) decrease are seen in 40-50% of patients with DM2. Three groups of factors are considered to be the basis of CKD development and progression in DM2: metabolic, hemodynamic, inflammation and fibrosis. Existing drugs that are used in patients with CKD and DM2 first of all target hemodynamic and metabolic disturbances, but their action against inflammation and fibrosis is indirect. Hyperactivation of mineralocorticoid receptors (MR) is considered as one of the main trigger factors of end-organ damage in patients with DM2 due to inflammation and fibrosis. Development of selective nonsteroidal MR antagonists (MRA) as a new class of medications is directed to demonstrate positive effects from blocking this pathophysiological pathway of CKD development and overcome the steroidal MRAs’ shortcomings. Hence pathophysiological hyperactivation of MR with subsequent inflammation and fibrosis in patients with CKD in DM2 is considered a promising therapeutic target for the new drugs with cardionephroprotective effect.
Today, the positive impact of bariatric surgery on the course of type 2 diabetes mellitus has been studied in detail. At the same time, not only the effect of direct weight loss and the incretin theory, but also other mechanisms for normalizing glycemia are being actively discussed. Thus, special attention is paid to the metabolism of bile acids and their influence on various indicators of homeostasis, including carbohydrate metabolism. After bariatric interventions of the bypass type, the passage of bile through the gastrointestinal tract, as well as its interaction with food masses, changes significantly, which served as the basis for studying this phenomenon. The information accumulated to date indicates enormous changes occurring not only in the anatomy, but also in the biology of the gastrointestinal tract after bariatric bypass surgery. The composition of the intestinal microbiota and the composition of bile masses undergo significant changes. Most of the works available today suggest that these changes are the cause of a number of metabolic rearrangements, and directly affect carbohydrate metabolism. This issue is still under study and accumulation of the necessary information, but today it can be stated with confidence that the role of bile passage, bile acid circulation and restructuring of the intestinal microbiota in the regulation of carbohydrate metabolism and energy balance after bariatric bypass surgery is of extreme importance.

Modern strategies for the treatment of type 2 diabetes mellitus involve the use of pathogenetically based approaches aimed at achieving optimal glycemic control and its long-term retention. Timely and rational use of 9 classes of hypoglycemic drugs, including as part of combination therapy, makes it possible to achieve significant success in diabetes therapy. One of the fundamental principles in the treatment of type 2 diabetes mellitus is the effect on insulin resistance. For this purpose, two groups of drugs are used: biguanides and thiazolidinediones (glitazones). The action of glitazones is directly related to an increase in the sensitivity of insulin-dependent tissues to insulin and a pronounced decrease in hyperinsulinemia in patients with type 2 diabetes. Of particular interest are the pathways of insulin signal transduction, the mechanisms of insulin resistance, and the possibilities of pathogenetic therapy with thiazolidinediones. Pioglitazone is currently the only available member of the thiazolidinedione class in the world, allowing to expand the management of diabetes mellitus by reducing insulin resistance in muscle and adipose tissue and glucose production by the liver. Its use can have a number of pleiotropic effects, including on cardiovascular diseases and non-alcoholic fatty liver disease, which expands the priorities for choosing hypoglycemic therapy in patients with type 2 diabetes at various stages of therapy.
Case report

Diabetes mellitus (DM) type 1 accounts for up to 90% of all cases of diabetes among children, adolescents and young adults (10 % are represented by T2DM, MODY, etc.). DM is characterized not only by glucose metabolism disorder, but also by abnormal protein and lipid metabolism, leading to severe macrovascular complications. A clinical case of diabetes type 1, hyperlipidemia, coronary artery disease (CAD) and chronic heart failure (HF) in a 25-year-old adult has been demonstrated. The medical examination revealed lipid metabolism disorders, multivessel coronary artery disease, which required myocardial revascularization, and severe heart failure with a reduced ejection fraction (HFrEF). The clinical case demonstrates that proper cardiovascular examination should be performed in all patients with diabetes and lipid disorders, regardless of age and type of diabetes. The authors also consider the use of sodium-glucose

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0).
ISSN 2072-0378 (Online)









































