


Original Studies
BACKGROUND: In 2018, a Frestyle Libre flash glucose monitoring system (FGM) appeared in Russia and became a potential alternative to the traditional CGM. Studies carried out to date have shown the advantages of FGM over SMBG, but only a few of them relate to real clinical practice, especially in children with type 1 diabetes.
OBJECTIVE: To evaluate the efficacy of FGM in children with T1DM in relation to glycemic control indicators, the occurrence of severe hypoglycemia and diabetic ketoacidosis, as well as the satisfaction of patients and their parents with the use of FGM.
MATERIALS AND METHODS: Single-center, prospective, observational cohort study. Children 4–18 years old with T1DM and HbA1c level less than 10.0% were invited to participate in the study on intensified insulin therapy (by MDI or CSII). The duration of the patient’s participation in the study was 6 months. At baseline and every 3 months thereafter, face-to-face consultations were conducted with an assessment of the general condition, HbA1c study, an assessment of glycemic indicators, progress in relation to glycemic control targets and correction of the therapy. A total of 228 patients (110 boys and 118 girls) who met the inclusion criteria were included in the study. The median age was 11.2 (8.6–14.7) years, the duration of type 1 diabetes was 3.8 (2–7.1), 136 patients received insulin therapy by CSII for 1.3 (0.8–2.6) years.
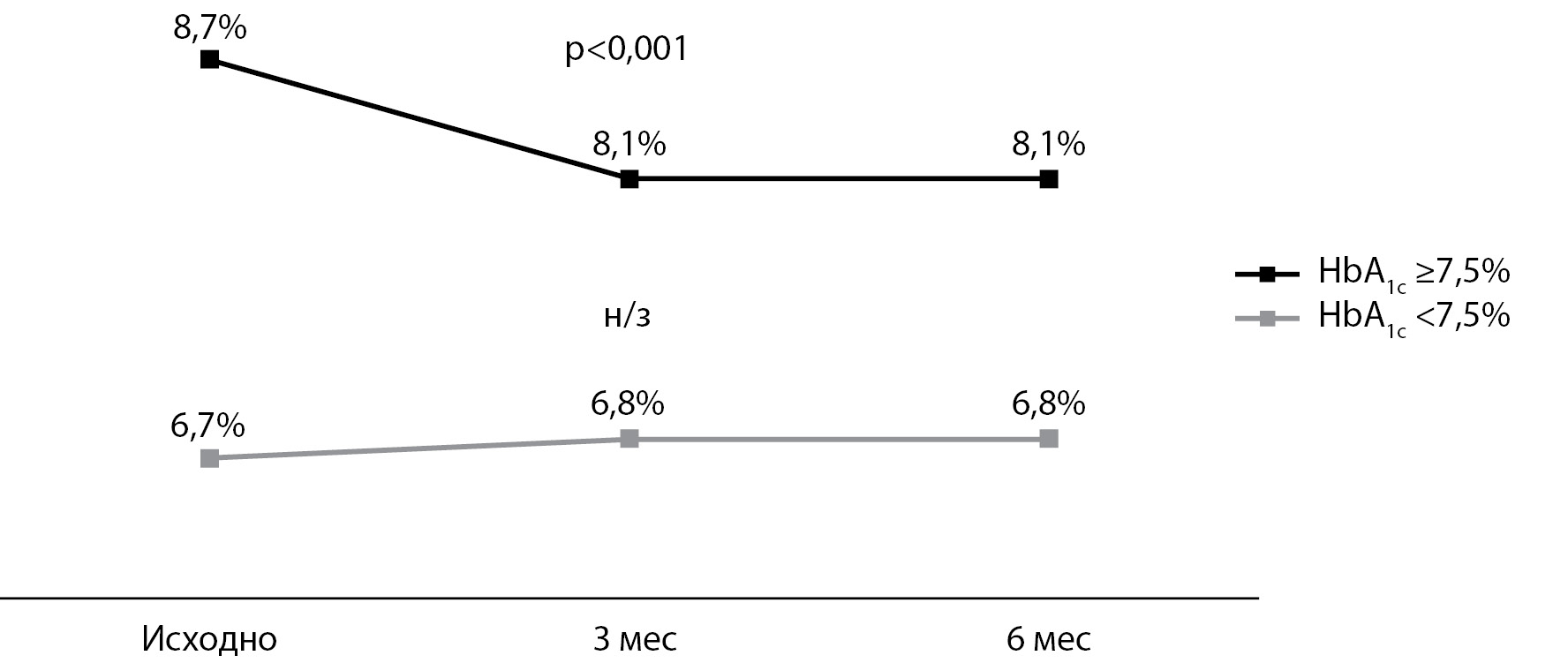
RESULTS: In the general group of patients, 3 and 6 months after the start of FGM use, the HbA1c values decreased statistically significantly by 0.2%. In addition, the number of children with HbA1c <7.5% increased by 6.1 and 4.9% at 3 and 6 months, respectively, but these changes were not statistically significant. The number of cases of DKA when using FGM decreased by 74%, and the number of cases of severe hypoglycemia by 83%, thus the number of episodes decreased by 4 and 6 times, respectively. Patients and / or their parents rated the ease of use and their experience with FGM on a scale from 0 (strongly agree) to 4 (strongly disagree). The majority of children and parents positively (0 or 1) assessed the convenience of installing and wearing the sensor (72.7–98.2%) using the FGM system in general (75.0–96.4%) and in comparison with the SMBG glucometer (92.3–98.2%).
CONCLUSION: The installation and use of FGM is convenient and comfortable for the vast majority of children and parents, while compared to SMBG, the use of FGM is more convenient and simpler, and glucose measurement is much faster and less painful.
BACKGROUND: «The vicious circle» of associations of diabetes mellitus (DM) with pancreatic pathology, when pancreatic diseases can initiate DM, and type 2 DM — cause functional and organic pancreatic pathology, determines the search for possible associations. Some studies have established a relationship between TNF or TP53 polymorphisms with DM or with pancreatic diseases.
AIMS: to determine and compare fasting plasma glucose and the frequency of hyperglycemia in patients with acute pancreatitis (APp), chronic pancreatitis (CPp), pancreatic cancer (PCp) depending on gender, etiology or stage of the disease, polymorphism -308G/A TNF gene in all patients, and polymorphism 72Arg/Pro gene TP53 in PCp..
MATERIALS AND METHODS: At the observational multicenter clinical cross-sectional uncontrolled case-study 44 APp, 97 CPp and 45 PCp were examined; the groups were comparable by sex/age. Informed consent form for participate in the study was obtained from all patients. The main outcome of the study: frequency of hyperglycemia in APp, CPp, PCp, considering the polymorphism TNF and TP53 genes.
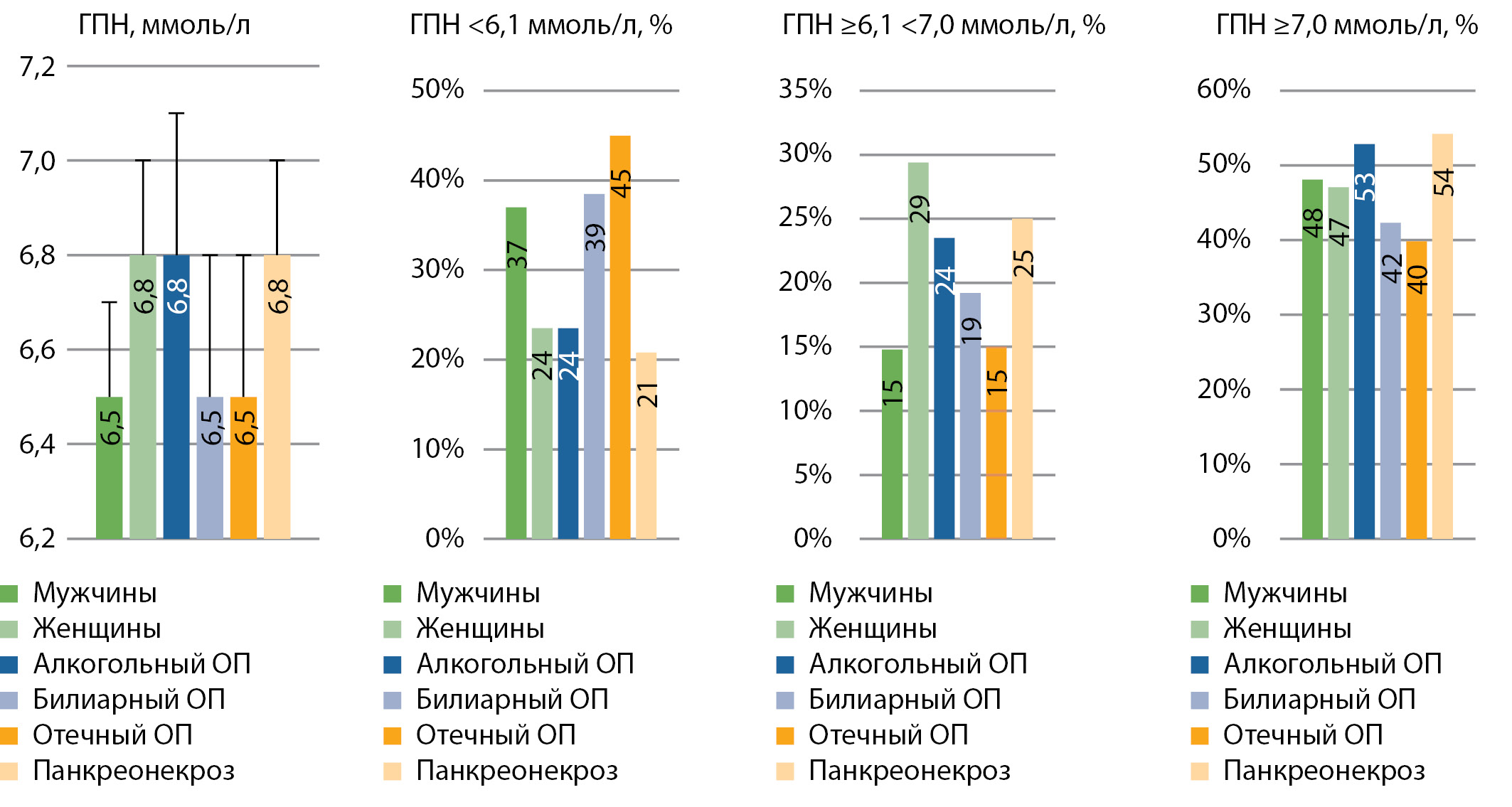
RESULTS: The lowest age-standardized fasting plasma glucose (FPG) was found in CPp (6,2±0,2 mmol/l) than in APp (6,7±0,2 mmol/l, p=0,041). In PCp (6,6±0,2 mmol/l), the average levels of FPG did not differ substantially when compared with APp (p=0,749) or CPp (p=0,092). In APp, the norm of GP was detected less frequently (31,8%) than in CPp (54,6%, χ2 =6,3, p=0,012), and the frequency of the norm of GP in PCp (48,9%) did not differ with that in APp or CPp. The frequency of FPG≥6,1<7,0 mmol/l did not differ in APp (20,5%), CPp (9,3%) or PCp (17,8%). The frequency of FGP≥7.0 mmol/l did not differ in APp CPp and PCp: 47,7, 36,1, 33,3%. Logistic regression analysis revealed a tendency for an increased chance of having stage 3–4 PC with FPG≥7,0 mmol/l (Exp (B)=3,205 95%CI 0,866–11,855, p=0,081) in PCp, but not in patients with pancreatic necrosis or “definite» СP.The frequencies of G/G (71,4, 74,7, 76,2%), G/A (26,2, 24,1, 23,8%) of TNF genotypes did not differ in APp, CPp or PCp, p>0,05. In PCp genotypes Arg/Arg, Arg/Pro, Pro/Pro polymorphism gene 72Arg/Pro TP53 in 2,4, 35,7, 61,9% of cases. No associations of GP≥7,0 mmol/l with TNF polymorphism in APp, CPp, PCp and with TP53 polymorphism in PCp were obtained.
CONCLUSIONS: The frequency of FGP≥7,0 mmol/l did not differ for various pancreatic disease and was not associated with the risk of pancreatic necrosis and “defined” CP. The -308G/A polymorphism TNF gene did not differ in APp, CPp or PCp and was not associated with impaired carbohydrate metabolism. The 72Arg/Pro polymorphism TP53 gene in PCp was not associated with impaired carbohydrate metabolism.
BACKGROUND: Gout is associated with a high incidence of type 2 diabetes mellitus (T2DM).
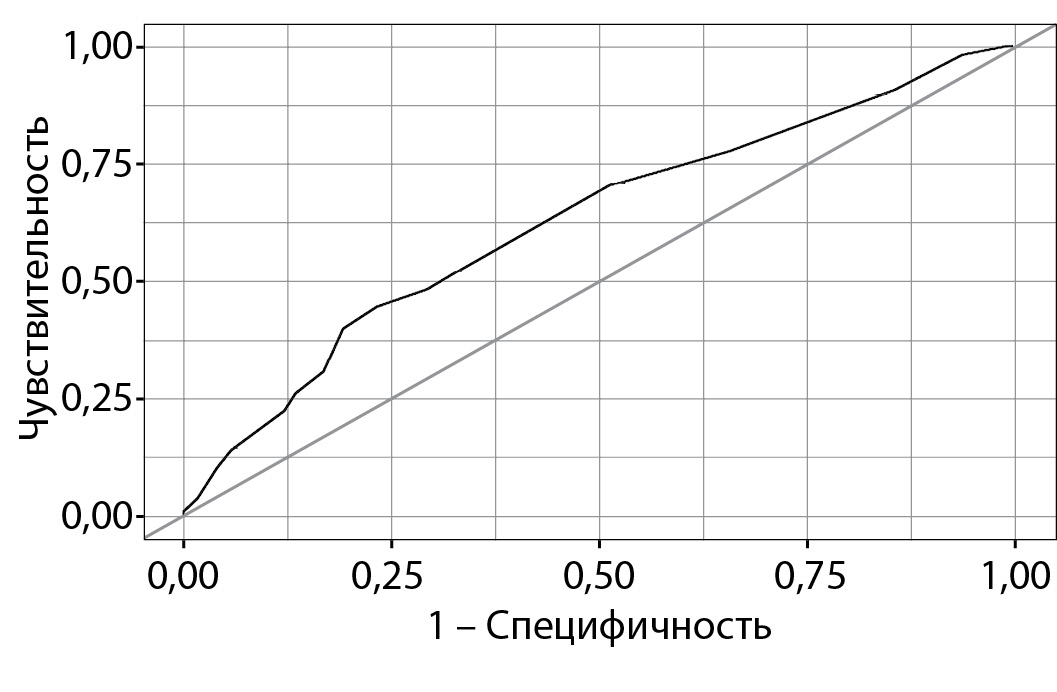
AIM: To calculate the risk of T2DM on the FINDRISС scale, to assess the sensitivity and specificity of the scale in patients with gout based on the results of prospective follow-up.
MATERIALS AND METHODS: A prospective single-center study included 444 patients with gout over 18 years of age (49 women, 395 men) without diabetes. The duration of follow-up ranged from 2 to 8 years. Initially, the risk of developing diabetes mellitus 2 was calculated according to the Russian version of the FINDRISС scale. The risk of developing T2DM was assessed as «low» with a total score (CC) <7 points, slightly increased — from 7 to 11 points, moderate — from 12 to 14 points, high — from 15 to 20 points, and very high — ≥20 points. To assess the validity of using the FINDRISС scale, an analysis of sensitivity, specificity, construction of the ROC curve with the determination of the area under the curve was carried out. The presence and number of subcutaneous tophi, the number of arthritis attacks over the last year, the number of affected joints during the illness, serum levels of creatinine, uric acid, hs-CRP, glycated hemoglobin were determined.
RESULTS: Over 5.66 [2.69; 7.64] years of follow-up, T2DM developed in 108 patients (24.3%). On the FINDRISС scale, low risk was found in 16 (4%), slightly increased in 187 (42%), moderate in 98 (22%), high in 80 (18%), very high in 63 (14%). The most common risk factors (RF) for T2DM included in FINDRISС were BMI> 25 kg / m2 — 85.6% of patients, taking antihypertensive drugs — 81.3% of patients, age over 45 years in 70.5% of patients. The sensitivity and specificity of the FINDRISС scale were 52.8% and 66.3%, respectively. According to these data, the quality of the model was assessed as moderate. 9% vs 31.1% (p = 0.014)), serum MK level ≤300 μmol / L. Developed type 2 diabetes 33.3% of patients with moderate / high / very high risk 18.1% of patients with low or slightly increased risk (p = 0.0002).
CONCLUSION: The FINDRISС scale can have sufficient sensitivity (52.8%) and specificity (66.3%) and can be used to calculate the risk of T2DM in patients with gout.
BACKGROUND: Disorders of carbohydrate metabolism are frequent complications after complex treatment of cancer. Early detection of these disorders allows to modify lifestyle, if necessary, apply drug therapy and correct the identified changes in time, which will subsequently lead to a decrease in cardiovascular risks, an improvement in the quality and an increase in the life expectancy of this group of patients.
AIM: To identify the frequency of occurrence and determine the optimal methods for early diagnosis of carbohydrate metabolism disorders in children after complex treatment of medulloblastoma.
MATERIALS AND METHODS: 97 patients (64 boys) were examined after complex treatment of medulloblastoma (surgical treatment, craniospinal radiation therapy [CSI], chemotherapy). The median age at the time of the survey was 11.2 (5.29 -17.9) years. The average follow-up period after the end of all types of treatment is 4.7 (0.59 - 11.94) years. At the time of examination, all patients were compensated for hypothyroidism and hypocorticism (if any), and no one was on growth hormone therapy. All patients underwent a standard oral glucose tolerance test (OGTT) and determination of the level of glycated hemoglobin (HbA1c).
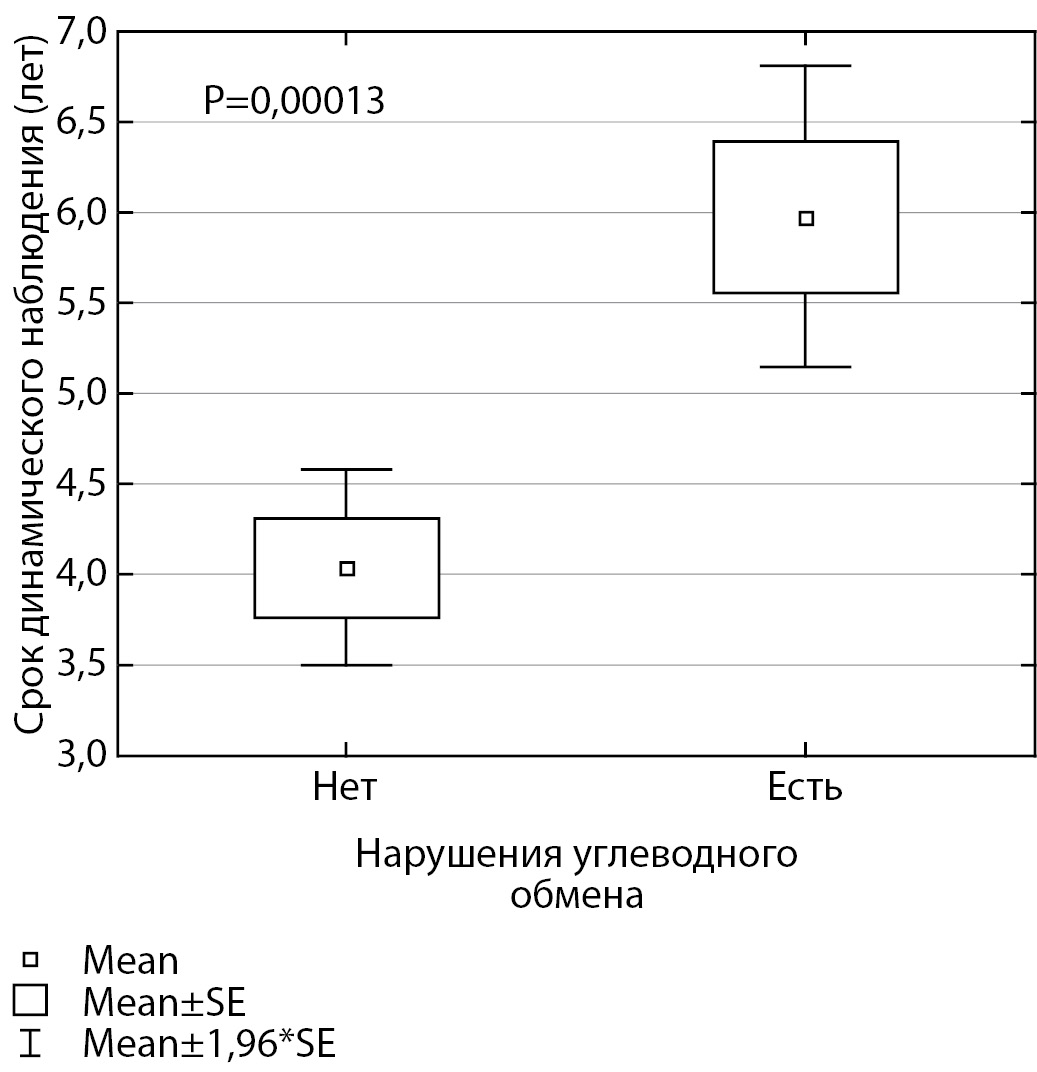
RESULTS: None of the patients had a basal glycemic level higher than 5.5 mmol / L. Impaired glucose tolerance ( glycemia at the 120th minute ≥7.8 mmol / L <11.09 mmol / L) was detected in 10 out of 97 patients (10.3%). 7 patients with IGT had insulin resistance (according to MATSUDA index), while 1 of them had normal HOMA-IR index. Only one patient with IGT had an increase in the level of glycated hemoglobin up to 6.2%. Insulin resistance (using the MATSUDA index) was present in 30 patients, and 11 of them had a normal HOMA-IR index. Thus, 34 out of 97 patients (35.1%) had disorders of carbohydrate metabolism (IGT and / or insulin resistance). At the same time, the level of glycated hemoglobin reflected disturbances in only one case, and the basal level of glycemia was not informative in any case.
CONCLUSION: Assessment of basal levels of glycemia and insulin, as well as glycated hemoglobin, is insufficient to exclude disorders of carbohydrate metabolism in patients after complex treatment of medulloblastoma. It is advisable to carry out a standard OGTT.
BACKGROUND: Type 2 diabetes mellitus (DM) is one of the important markers for the development of adverse cardiovascular events after carotid endarterectomy (CEE). However, studies on this issue are based on small sample of patients and do not take into account the type of surgery as an additional factor of potentially negative impact on the course of the postoperative period.
AIM: Analysis of hospital and long-term results of eversion and classical CEE with plastic surgery of the reconstruction zone with a biological patch in patients with type 2 diabetes and without it.
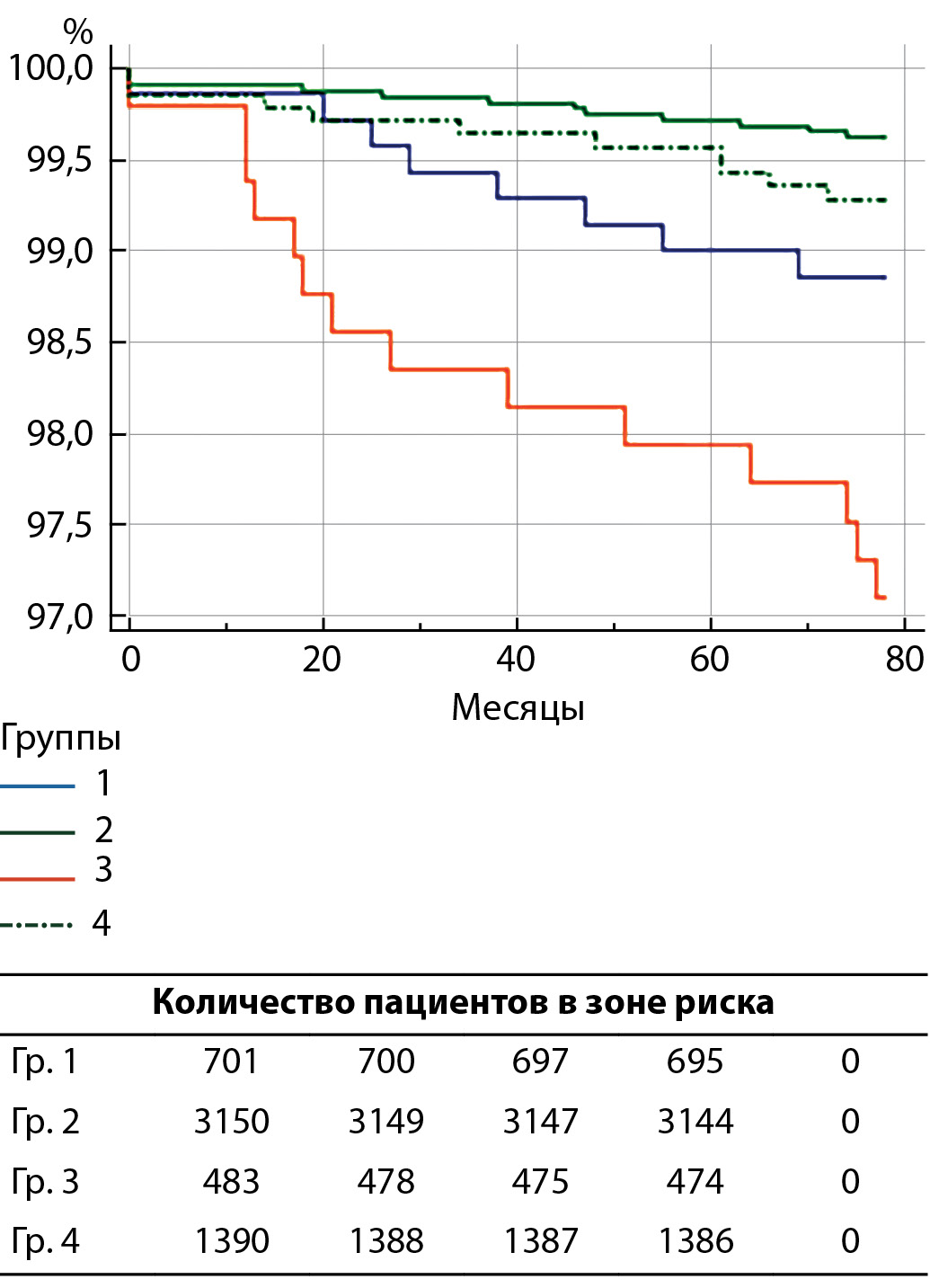
MATERIALS AND METHODS: In this multicenter retrospective study from January 2010 to December 2020. included 5731 patients. Depending on the presence / absence of type 2 diabetes and the type of implemented CEE, 4 groups were formed: group 1 — 12.2% (n = 702) — patients with type 2 diabetes and eversion CEE; Group 2 — 55.0% (n = 3153) patients without type 2 diabetes and eversion CEE; Group 3 — 8.5% (n = 484) patients with type 2 diabetes and classical CEE; Group 4 — 24.3% (n = 1392) patients without type 2 diabetes and classical CEE. The duration of postoperative follow-up was 78.6 ± 39.2 months.
RESULTS: At the long-term follow-up stage, patients with type 2 diabetes after the classical surgical technique demonstrated the highest rates of all types of complications: death (p <0.0001), MI (p = 0.011), ischemic stroke (p <0.0001), restenosis / occlusion of the ICA (p <0.0001), combined end point (p <0.0001). At the same time, the group of eversion CEE with impaired carbohydrate metabolism took the second position in terms of the prevalence of adverse events. These circumstances demonstrate that patch implantation is accompanied by an increased risk of developing not only myocardial infarction, but also restenosis of the reconstruction zone, as well as the associated ischemic stroke, which was demonstrated by our results.
CONCLUSION: Patients with type 2 diabetes and a history of CEE are at increased risk of ischemic stroke at the hospital stage of observation and all unfavorable cardiovascular conditions (death, myocardial infarction, ischemic stroke, restenosis or ICA occlusion in the reconstruction zone) in the long-term postoperative period.
INTRODUCTION: The prevalence of diabetic foot syndrome is increasing in the Indian population. It is a triad of neurological, vascular, and biomechanical changes due to long term diabetes mellitus (DM). Altered plantar pressure distribution is a risk factor for developing diabetic foot ulcers. The purpose of this study is to evaluate the altered plantar pressure distribution in diabetic peripheral neuropathy individuals with peripheral vascular disease in comparison with diabetic peripheral neuropathy and non-diabetic neuropathy. Therefore, the objective of the study is to evaluate the plantar pressure distribution and parameters in type 2 DM (T2DM) with diabetic foot syndrome.
METHODS: In this study, 60 participants with T2DM were recruited in either one of the three groups: 20 Diabetic non-neuropathy (DNN), 20 Diabetic peripheral neuropathy (DPN), and 20 Diabetic peripheral neuropathy with the peripheral arterial disease (DNPAD). Then we compared the plantar pressure parameters like maximum plantar pressure, pressure-time integral, fore foot-hind foot ratio, and total contact area were measured using a WinTrack plantar pressure system.
RESULTS: The diabetic peripheral neuropathy with peripheral vascular disease group shown a significant difference in all the plantar pressure parameters measured in comparison with the diabetic peripheral neuropathy group. There was increased Maximum plantar pressure, pressure-time integral and forefoot hindfoot ratio, and reduced total contact area of the foot (p < 0.05).
CONCLUSION: For patients, with combined peripheral neuropathy and peripheral vascular disease have increased plantar pressure distribution, are at higher risks of developing neuro-ischemic foot, which further leads to diabetic foot ulcers.
Review
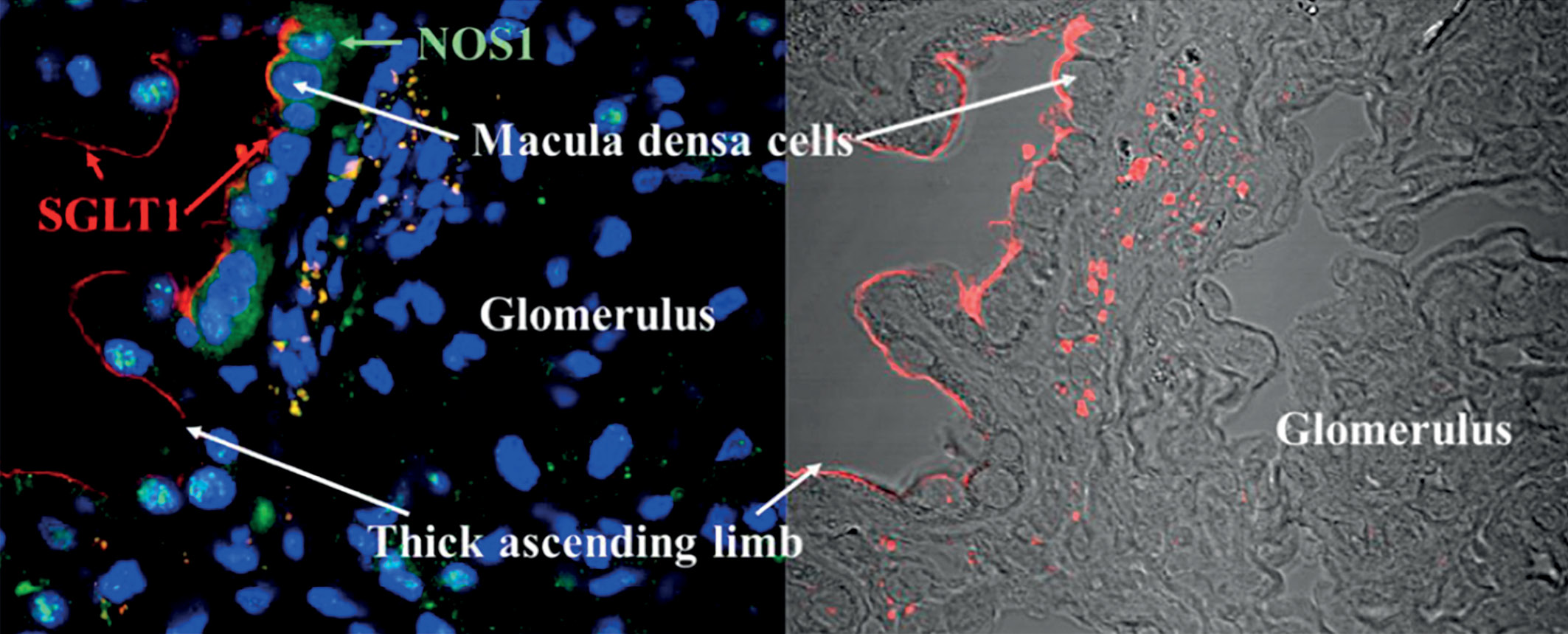
The series of the cardiovascular outcome trails have demonstrated the nephroprotective properties of the gliflozins. Canagliflozin in the CREDENCE, which was the first study with a primary focus on the evaluation of the nephroprotective properties of gliflozin, have demonstrated the possibility to slow the progression of the renal disease. The paper summarizes the additional data from the CREDENCE trail: assessment of the efficacy of canagliflozin by initial eGFR; efficacy in individuals with GFR <30 ml/min/1.73 m2 ; long-term effects of canagliflozin on anaemia-related outcomes; effects of canagliflozin on serum potassium; effects on heart failure and cardiovascular mortality. There are discussed the current treatment algorithms for patients with type 2 diabetes and CKD where using of gliflozins is a priority option. Canagliflozin is a drug with a relatively low ratio of SGLT1/SGLT2 selectivity. The effects of the inhibition of SGLT1 transport in the kidney and in the intestine are described and their additional influence on reducing of the postprandial glycemia and additional nephroprotection.
Type 2 diabetes prevalence is increasing dramatically worldwide. Conservative therapy doesn’t bring stable effect and is often insufficient, not to mention the lack of prospects to cure the disease. Fortunately, accumulating evidence points towards the notion that a complete remission of type 2 diabetes is feasible following a choice of surgical interventions. The efficacy of bariatric surgery in particular for achieving glycemic control has highlighted surgery as a candidate curative intervention for type 2 diabetes. When compared to intensive medical therapy and lifestyle intervention, metabolic surgery has shown superiority in achieving reducing number of medications and metabolic factors improvement, which translates in long-term benefits on diabetes progression and complications. Understanding factors that predict diabetes remission can help to select patients who will benefit most from bariatric surgery and to choose the most effective type of operation. This literature review analyzes studies of the most significant clinical and biochemical predictors of remission of type 2 diabetes mellitus after bariatric interventions, as well as highlights well-known mathematical prediction models.
Metformin is one of the most commonly prescribed drugs for the treatment and prevention of type 2 diabetes mellitus (T2DM). Numerous evidence accumulates indicating that both genetic and environmental factors underlie adverse side effects of metformin, as well as individual differences in patient response to treatment The present review summarizes information on genetic factors and environmental modifiers determining patients’ individual response to metformin treatment. The data on the role of polymorphism of the most significant genes and protein products encoded by them both in the development of adverse effects and in determining the therapeutic response are summarized, and the place of metformin in the realization of the phenotypic effects of these genes is discussed.
Endogenous conditions and exogenous effects modifying the response to metformin are considered. Among them are factors that affect the functional state of the genome (the level of methylation of genes, one way or another associated with the response to metformin, etc.), reflecting the biological characteristics of the organism (gender, age), health level (the presence of concomitant diseases, the supply of biometals and vitamins), taking other medications, etc. Thus, there is a wide range of factors modifying the response to metformin, which, unlike genetic characteristics, are largely controllable. At the same time, both genetic and environmental factors may differ in significance in different ethno-territorial groups of the population. This information should be taken into account when developing a personalized approach to prescribing metformin for the treatment of type 2 diabetes, as well as when recommending its use for the treatment of other diseases.

Recent studies have shown a strong direct correlation between fasting insulin levels and cancer mortality in men. This may be especially true in patients over 65, who are, in the first place, more likely to develop prostate cancer than younger patients. It should be noted that it is insulin, and not glucose, that is associated with the claim for the development of cancer. Hyperinsulinemia, which often occurs as a result of androgen deprivation therapy (ADT), the standard treatment for prostate cancer, is associated with a high tumor aggressiveness and faster treatment failure — the development of castrate-refractory prostate cancer. It is reasonable to assume that hyperinsulinemia — under whatever circumstances it is caused, whether due to ADT or due to inadequate nutrition and other lifestyle factors — can have the same negative effect on cellular signaling.
Metabolic syndrome — essentially chronically elevated insulin levels — is closely associated with recurrence of cancer and worse post-treatment outcomes, which has led researchers to question generally accepted dietary guidelines for cancer patients, especially when they are undergoing treatment or recover from treatment, which may include recommendations to consume anything that will help maintain or restore body weight, regardless of sugar or carbohydrate content or its effect on insulin levels. A large number of patients live with hyperinsulinemia, but normoglycemia. Chronic hyperinsulinemia is the main driver of cardiometabolic disease, even when blood sugar levels are within reference values. The scale of this problem is not recognized by the medical and scientific community.

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0).
ISSN 2072-0378 (Online)









































