



ORIGINAL STUDIES
BACKGROUND: Binge eating disorder (BED) is the most prevalent eating disorder in the population, poorly studied in patients with Type 2 diabetes mellitus (T2DM). There are no generally accepted guidelines on pharmacological treatment of BED and no studies with more than 3-month duration. Glucagon-like peptide 1 receptor agonists (GLP1RA) could be a promising class of agents for the treatment of BED in T2DM patients due to their effects on central mechanisms of appetite and satiety regulation.
AIM: To assess efficacy and safety of GLP1 RA for treatment of BED in patients with T2D.
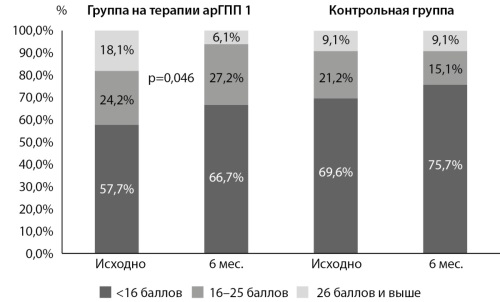
METHODS: Sixty six outpatients with T2DM and BED participated in this pilot open-label prospective comparative study of 6 mo’ duration followed by a 6 mo follow-up after GLP1RA withdrawal. All 66 continued their previous anti-hyperglycemic agents, 33 patients (50%) were prescribed a GLPRA (dulaglutide, or semaglutide, or lixisenatide combined with glargin). Thirty three patients were in the control group without GLPRA. In addition to standard clinical and laboratory examinations, all patients completed tests/questionnaires for assessment of their quality of life, depression, stait/trait anxiety, alexithymia and other personality characteristics, and physical complaints. Changes in BED severity and all other parameters were assessed at 3 and 6 months, and BED severity only was assessed at 6 months after the end of GLP1RA.
RESULTS: After 6 months of GLP1RA therapy, 63,6% of the patients were in complete remission of BED (р<0,001), 36,3% were in partial remission, and complete form of BED was absent (0%). Along with BED improvement, there was a decrease of body weight from 106,3±17,6 to 98,9±17,2 kg at 6 months (р<0,00001), waist circumference from 118,1±12,5 to 110,1±12,0 cm (р<0,00001), and HbA1c levels by 1,2% from the baseline (р=0,0005). Improvement of BED was associated with positive changes of some psychological parameters, such as depression, hypochondriasis, general (but not diabetes-related) quality of life and psychosomatic complaints. In the control group, BED severity, anthropometric, metabolic, and psychological characteristics remained unchanged. At 6 months, most of the parameters studied in the GLP1RA group were significantly better than in the control. No patients withdrew from the study due to adverse events of GLP1 RA. At 6 months after GLP1RA withdrawal, BED relapsed in all patients.
CONCLUSION: GLP1 receptor agonists are effective, safe and well tolerated in the treatment of BED in Type 2 diabetes patients. They facilitate the achievement of the main goal of BED treatment (complete or partial remission of BED) in 100% of the cases with marked improvements in metabolic and a range of psychological parameters.
BACKGROUND: The study of the clinical and epidemiological characteristics of any pathology in regions with a centralized medical care system is very informative. Thus, the Republic of Sakha (Yakutia) is very interesting for conducting epidemiological studies in view of the possibility of accounting for all cases of diabetes in children in the Department of Pediatric Endocrinology and Gastroenterology of the Pediatric Center of the Republic hospital № 1 — the National Center of Medicine named after M.E. Nikolaev (RH№1 — NCM named after M.E. Nikolaev), the population of the region is ethnically heterogeneous.
OBJECTIVE: To study the clinical and epidemiological characteristics of type 1 and type 2 diabetes mellitus in the Republic of Sakha (Yakutia).
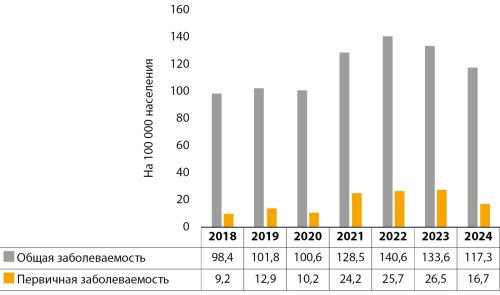
MATERIALS AND METHODS: The article describe the clinical and epidemiological characteristics of type 1 and type 2 diabetes in children in the Republic of Sakha (Yakutia). According to official statistics, an increase in the incidence of diabetes mellitus in children has been revealed in the period from 2018–2024.
RESULTS: According to the data of the republican registry of the Department of Endocrinology and Gastroenterology of the Pediatric Center of the RH№1 — NCM named after M.E. Nikolaev, the age of the debut, the ethnic characteristics of the patient population, age-sex characteristics and features of therapy were determined. Over the past 7 years, the Republic of Sakha (Yakutia) has seen a steady increase in the incidence of type 1 and type 2 diabetes among children aged 0–17 years. Yakut and Russian children suffer from type 1 diabetes equally often, and Yakut children mostly suffer from type 2 diabetes. The age of onset of type 1 diabetes is 10–14 years, and girls are more likely to be ill. 90% of children at the onset of type 1 diabetes are admitted in a state of ketoacidosis. In the treatment of type 1 diabetes, a combination of insulin analogues is used, with type 2 diabetes mainly metformin.
CONCLUSION: The clinical and epidemiological situation of diabetes mellitus in children and adolescents in the Republic of Sakha (Yakutia) requires special attention and the adoption of new organizational measures within the framework of federal and regional programs.
BACKGROUND: structural and morphological changes in the heart in young patients with type 1 diabetes mellitus occur at the preclinical stage of cardiovascular disease and worsen the cardiovascular prognosis in this group of patients. Myocardial fibrosis is one of the main factors influencing ventricular myocardial stiffness and the development of heart failure. The search for early markers of myocardial remodeling, among which microRNAs are of particular interest, will improve diagnosis and reduce the risk of cardiovascular complications.
OBJECTIVE: to study the expression levels of individual microRNAs involved in myocardial remodeling processes in young patients with type 1 diabetes mellitus.
MATERIALS AND METHODS: the study was conducted at the Federal State Budgetary Institution “I.I. Dedov National Medical Research Center of Endocrinology” of the Ministry of Health of the Russian Federation. The study included 110 participants without cardiovascular disease, divided into 2 groups: 80 patients with type 1 diabetes (the study group) and 30 individuals without type 1 diabetes (control group). All participants underwent a general clinical examination, bioimpedance analysis, electrocardiography, cardiac MRI with T-1 mapping technology (used for quantitative assessment of myocardial fibrotic changes, extracellular volume fraction, and construction of pixel-wise heart structure maps), ergospirometry, and assessment of circulating miR-126-5p and miR-21-5p expression levels.
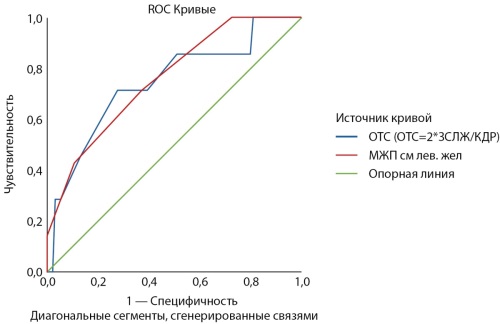
RESULTS: in the group of patients with type 1 diabetes, examination revealed signs of myocardial remodeling: сardiac MRI revealed thickening of the interventricular septum (p=0.028), left ventricular posterior wall (p=0.012), and left ventricular relative wall thickness (p<0.001), compared with individuals without type 1 diabetes. Additionally, patients with type 1 diabetes demonstrated significantly lower levels of cardioprotective miR-126-5p (p=0.046). It is noteworthy that 8.7% of patients in the type 1 diabetes group had fibrous tissue in the myocardium. No such patients were detected in the control group.
CONCLUSION: cardiac MRI with late gadolinium enhancement is significantly more sensitive than echocardiography in detecting diffuse myocardial fibrosis, which indicates an unfavorable cardiovascular prognosis. In this study, diffuse myocardial fibrosis was detected by cardiac MRI in 8.7% of patients with type 1 diabetes. The group of type 1 diabetes patients with diffuse myocardial fibrosis was characterized by more pronounced initial structural myocardial changes (according to echocardiographic data). Patients with type 1 diabetes demonstrate lower levels of cardioprotective microRNA — miR-126-5p.
BACKGROUND: treatment of patients with the persistent form of atrial fibrillation (AF) is an unsolved problem of the healthcare system due to a high risk of disability and mortality. Considering a low effectiveness of drug treatment for AF, intervention treatment (catheter ablation) is the main technology for eliminating trigger activity of pulmonary veins. The frequency of AF recurrence of patients with diabetes mellitus (DM) after surgery is higher than of patients without disorders of carbohydrate metabolism what could be explained with non-pulmonary vein triggers on the posterior wall of the left atrial (LA). Opportunities of preoperative diagnostic of non-pulmonary vein triggers of AF and personalization of catheter ablation reports of patients with DM has not been determined yet.
AIM: to estimate an opportunity of preoperative diagnostic of rotor activities for personalization of catheter ablation reports of patients with the persistent form of AF and DM.
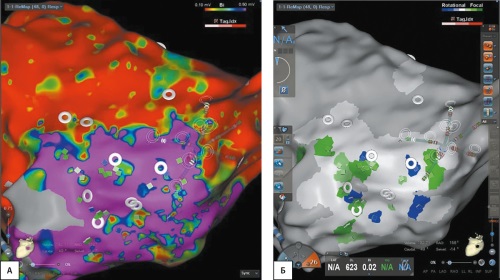
MATERIALS AND METHODS: the study included 25 patients with persistent form of AF. Group 1: patients with DM aged 58–77. Group 2: patients without DM aged 38–76. To determine treatment tactics, all patients were made noninvasive electrophysiological mapping with the construction of a personalized virtual cardiac phantom. All patients were undergone interventional treatment.
RESULTS: taking into account the identified localizations of rotor activity, the interventional treatment protocol was optimized: radiofrequency catheter isolation of PV was supplemented with focal (32%), linear (20%), and combined (focal+linear; 4%) radiofrequency effects.
Extrapulmonary rotor activity was more common in patients with DM than in patients without diabetes.
CONCLUSION: non-invasive electrophysiological mapping of the heart with the construction of a virtual heart phantom allows to verify rotor activity in the LA.
In patients with diabetes type 2 and persistent AF rotor activity is more common than in patients without carbohydrate metabolism disorders (p<0.001). Personalization of the catheter ablation protocol in the left atrium based on rotor activity marked during pre-surgery examination helps to improve long-term results of maintaining sinus rhythm.ividual microRNAs involved in myocardial remodeling processes in young patients with type 1 diabetes mellitus.
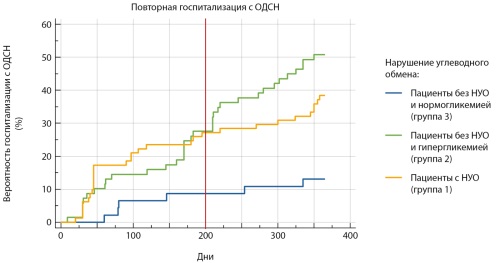
BACKGROUND. The prevalence of chronic heart failure (CHF) and carbohydrate metabolism disorders (CMD) is steadily increasing in the 21st century. Currently, research into the role of stress hyperglycemia in the prognosis of patients with acute decompensated heart failure (ADHF) is relevant, given significant changes in diagnostic capabilities and drug therapy.
AIM. To determine the prognostic role of stress hyperglycemia in ADHF in patients with different carbohydrate metabolism status.
MATERIALS AND METHODS. The study included 200 patients diagnosed with ADHF. The participants were divided into 3 groups: group 1 — patients with a previously established diagnosis of CMD; group 2 — patients who had increased glucose levels during hospitalization above 6.1 mmol/L on an empty stomach and/or above 7.8 mmol/L at any time during the day, without a diagnosis of CMD; group 3 — patients without CMD in whom hyperglycemia was not recorded. A comparative analysis of clinical and anamnestic data, instrumental and laboratory parameters at the hospital stage was carried out. We assessed outcomes one year after the episode of ADHF, including rehospitalization due to ADHF after discharge and all-cause mortality.
RESULTS. Patients with stress hyperglycemia were younger than those with CMD, were more often male, and less likely to have arterial hypertension and coronary artery disease. During the first 200 days of follow-up, rehospitalization rates due to ADHF were comparable between the groups with CMD and stress hyperglycemia (p=0.18). Starting from day 200, worse outcomes were observed in the stress hyperglycemia group (p=0.03; RR 2.45, 95% CI 1.08–6.56). Patients with stress hyperglycemia more often suffered from atrial fibrillation and had lower left ventricular end-diastolic index and left ventricular end-systolic index compared with the group without CDM and normoglycemia. Patients with stress hyperglycemia were more often hospitalized with recurrent ADHF during the entire period compared with patients without CMD and registered hyperglycemia (logrank test p<0.001; RR 3.5 CI 1.9–6.5).
CONCLUSION. Stress-induced hyperglycemia in patients with ADHF is an important risk factor for worsening heart failure prognosis. Patients with hyperglycemia during ADHF require closer monitoring and control of carbohydrate metabolism indicators within one year after hospitalization.
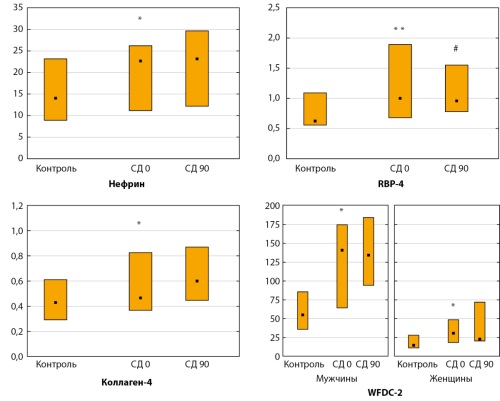
BACKGROUND: Sodium-glucose cotransporter 2 (SGLT2) inhibitors have been implemented into the treatment standards for chronic kidney disease (CKD) in patients with type 2 diabetes (T2D). Identification of predictors of the protective effect of SGLT2 inhibitors on the kidneys remains an urgent task.
AIM: To evaluate the effects of the SGLT2 inhibitor empagliflozin on the levels of biomarkers of renal injury, fibrosis and low-grade inflammation in patients with T2D with CKD and/or high cardiovascular risk.
MATERIALS AND METHODS: This prospective cohort single-center study included 30 patients with T2D newly initiated treatment with an SGLT2 inhibitor. Before and on day 90 of treatment with empagliflozin (10 mg/day), urinary excretion of nephrin, retinol-binding protein 4 (RBP-4), type IV collagen, and fibrosis marker WFDC-2, as well as serum concentrations of high-sensitivity C-reactive protein (hsCRP) and tumor necrosis factor receptor 1A alpha (TNFRSF1A) were determined by ELISA. Twenty healthy individuals were included in the control group.
RESULTS: Patients with T2D compared to controls initially demonstrated higher excretion of nephrin (p=0.03), RBP-4 (p=0.001), type IV collagen (p=0.04) and WDFC-2 (p=0.02), as well as higher serum concentrations of hsCRP and TNFSF1A (p=0.03). Empagliflozin treatment was associated with a significant decrease in the excretion of RBP-4 (p=0.04) and TNFRSF1A levels (p<0.001). Excretion of nephrin, type IV collagen, WFDC-2 and hsCRP levels did not change significantly (p>0.05). Baseline RBP-4 excretion and serum TNFRSF1A levels were associated with changes in creatinine levels during empagliflozin treatment.
CONCLUSION: In patients with T2D with CKD and/or high cardiovascular risk, empagliflozin treatment resulted in decreased urinary excretion of RBP-4 and serum TNFRSF1A levels. These data may indicate a protective effect of empagliflozin on tubular dysfunction and low-grade inflammation.
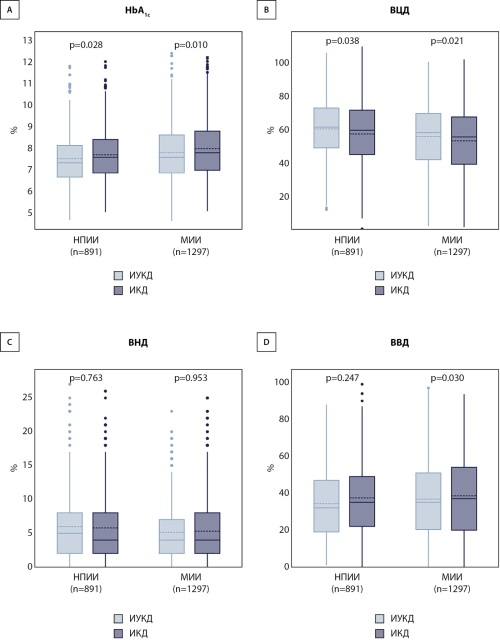
BACKGROUND: Fast-acting insulin aspart has superior pharmacokinetic properties compared to traditional rapid-acting insulin analogs, but data on its real-world clinical effectiveness in children and adolescents are limited
AIM: To evaluate the effectiveness of fast-acting insulin aspart compared to rapid-acting insulin analogs in children and adolescents with type 1 diabetes (T1D) under real-world clinical practice conditions.
MATERIALS AND METHODS: A cross-sectional study of 2,188 children and adolescents with T1D aged 1–18 years was conducted. Primary outcomes included glycated hemoglobin (HbA1c) level and time in range (TIR, 3.9–10.0 mmol/L). Statistical analysis involved the Mann-Whitney U test for between-group comparisons and multivariate linear regression to assess independent predictors of outcomes.
RESULTS: The median age of participants was 12.0 [9.0; 15.0] years, with diabetes duration of 4.3 [2.3; 7.1] years. Multivariate analysis confirmed an independent association of fast-acting insulin with 0.182% lower HbA1c (95% CI: -0.292; -0.071, p=0.001) and 2.663% higher TIR (95% CI: 1.031; 4.294, p=0.001) after adjustment for age, diabetes duration, and insulin delivery method. The most pronounced benefits were observed in adolescents aged 13–18 years and patients with diabetes duration exceeding 7 years.
CONCLUSION: Fast-acting insulin aspart demonstrates statistically significant and clinically relevant advantages in glycemic control among children and adolescents with T1D in real-world clinical practice, supporting its broader use in pediatric populations.
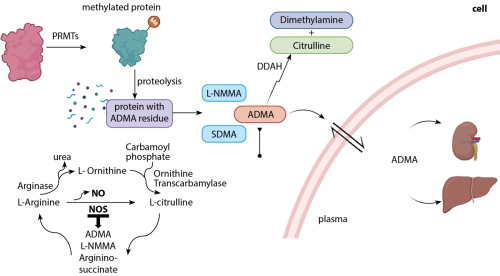
BACKGROUND. Type 2 Diabetes Mellitus (T2DM) is a primary public health concern globally, characterized by chronic hyperglycemia, insulin resistance, impaired beta-cell function. Endothelial dysfunction is a hallmark of diabetes and is exacerbated by hyperlipidemia.
AIM. This study investigates the impact of hyperlipidemia on nitric oxide synthesis, arginine metabolism, and vascular health markers in T2DM.
MATERIALS AND METHODS. A total of 120 participants were included in this cross-sectional, comparative study. Serum methylarginine derivatives (Asymmetric dimethyl arginine (ADMA), Symmetric dimethyl arginine (SDMA), L-N Mono-methylarginine (L-NMMA) and related metabolites (arginine, homoarginine, citrulline, ornithine) levels were measured in three groups: diabetes with hyperlipidemia (DM-HL), diabetes with normolipidemia (DM-NL), and healthy controls (HC) using API SCIEX 3200 LC-MS/MS methods. Statistical comparisons between groups were performed using IBM SPSS 26.0 to assess the influence of hyperlipidemia on these markers.
RESULTS. ADMA and SDMA levels were significantly elevated in DM-HL group compared to DM-NL and HC (p=0.001, p=0.000 respectively), indicating increased endothelial dysfunction and potential dyslipidemia-induced renal or vascular impairment. Reduced arginine and homoarginine levels in diabetic groups suggest impaired nitric oxide synthesis and altered urea cycle function (p=0.013, p=0.000 respectively). Notably, the DM-HL group exhibited significantly higher L-NMMA levels (p=0.001). It disrupted metabolic ratios (e.g., SDMA/ADMA, arginine/ADMA, and homoarginine/ADMA), reflecting enhanced nitric oxide inhibition and reduced bioavailability. Hyperlipidemia significantly exacerbated these disruptions, as evidenced by altered citrulline/arginine and citrulline/ADMA ratios, underscoring its additive impact on endothelial dysfunction.
CONCLUSIONS. Hyperlipidemia amplifies the adverse effects of diabetes on endothelial function by exacerbating nitric oxide inhibition, oxidative stress, and arginine metabolism dysregulation. Key biomarkers and metabolic ratios, particularly ADMA and SDMA-related indices, provide valuable insights into cardiovascular risk in this population. Therapeutic strategies targeting lipid management, arginine supplementation, and ADMA reduction could improve vascular health and mitigate cardiovascular complications in DM-HL.
REVIEWS
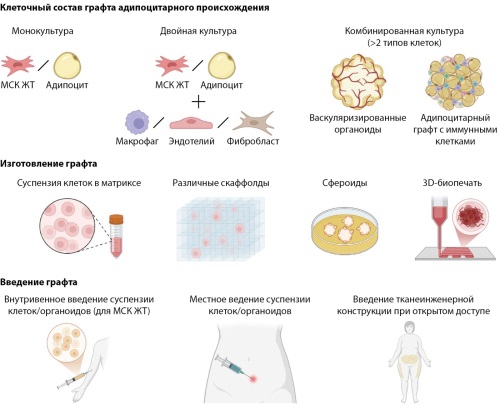
Metabolic diseases are currently significant factors of disability and mortality in the Russian Federation. Modern pharmacology offers many tools for glycemic control, but their effects on weight loss in patients are limited. There is currently no therapy for lipodystrophies except for symptomatic therapy. In this regard, the development of tissue engineering in combination with genetic technologies is a key factor in creating new approaches to the treatment of metabolic diseases. The presented review article describes various approaches to tissue engineering for the formation of grafts of adipocyte origin. Today, a variety of cells are used for these purposes — these are adipose-derived mesenchymal stromal cells (ADSC), which are progenitors of mature adipocytes and components of the cellular niche of adipose tissue, and metabolically healthy adipocytes, and thermogenic adipocytes. Cells are used both in a native state and can be genetically modified. The presented review integrates knowledge about transplantation of various adipose tissue derivatives in different tissue-engineered formats for the treatment of major metabolic diseases, which include lipodystrophies, obesity, and type 2 diabetes mellitus. The results of the review can give a significant impetus to the development of new approaches to the treatment of metabolic diseases.
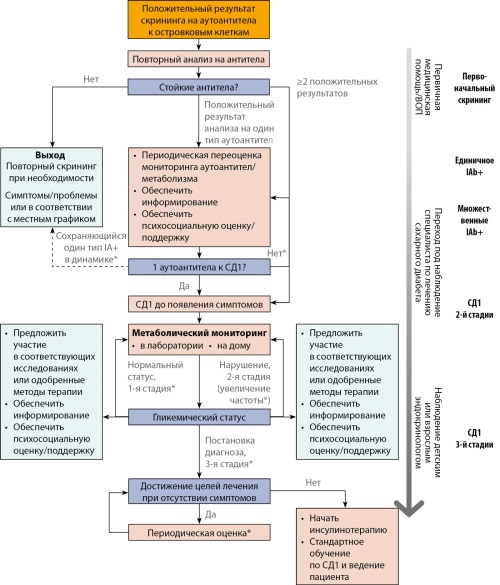
Type 1 diabetes is an autoimmune disease that causes damage and destruction of the pancreatic islet beta cells, leading to insufficient insulin production, followed by metabolic disturbances and clinically overt hyperglycemia, which requires lifelong insulin therapy. Currently, it is possible to detect the disease at preclinical stages, when pancreatic islet beta-cell function is sufficient to prevent hyperglycemia and the need for insulin therapy, by determining antibodies to islet cells (ICA, IA-2, GAD, IAA, Zn8T). Due to the high relevance and growing demands from the medical community regarding the problem of early diagnosis of T1D and the need to standardize approaches, several international guidelines on screening and monitoring individuals with positive autoantibodies (AAb) at preclinical stages of T1D were published during 2024. Monitoring these patients will reduce the risk of DKA, give them and their families more time to acquire knowledge and skills for diabetes management, and may also reduce anxiety and stress associated with the onset of the clinical stage of T1D. This review analyzes and compares international approaches to screening and monitoring the preclinical stages of T1D.
CASE REPORTS
Insulin resistance (IR) type A is an autosomal dominant condition with a prevalence of 1/100 thousand people. It’s associated with a defect in the insulin receptor gene INSR. It’s more often diagnosed among young women due to hyperandrogenism. In men, the disease is usually diagnosed only after they develop diabetes mellitus.
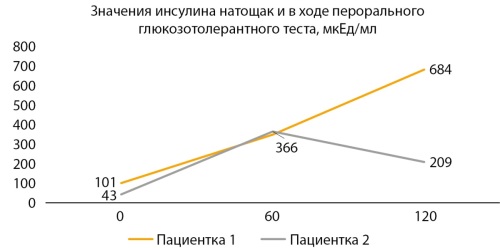
The article presents clinical cases reports of IR type A in an adolescent girls with no obesity and prediabetes and diabetes. Patient 1, 17.9 years old presented complaining of acne, darkening of the skin on armpits, back of the neck, groins, elbows, inner thighs. Her fasting insulin was 101 µed/ml (HOMA-IR 18,9). 2 hours after glucose loading insulin was at the level of 684 µed/ml. Patient 2 — 16.6 years old, presented with the complaints of an irregular menstrual cycle of up to 90 days. She had no excess weight (SDS BMI = -0.7 SD). Multiple skin papillomas were observed. Laboratory and ultrasound signs of polycystic ovary syndrome were revealed, as well as normoglycemia and severe IR (up to 366 μU/ml during oral fasting glucose tolerance test). In both patients, the diagnosis was confirmed by the results of genetic testing. Patient 1 was diagnosed with a pathogenic heterozygous defect in exon 19 of the INSR insulin receptor gene (NM 000208.4, ch19:7122707C>T, c.3436G>A), leading to an amino acid substitution at protein position 1146 (p.Gly1146Arg). Patient 2 revealed a heterozygous variant unknown clinical significance in exon 17 of the INSR gene (NM 000208.4) c.3095G>A (HG38, chr19:7125446C>T), leading to the amino acid substitution of glycine for aspartate at position 1032 (p.Gly1032Asp). Metformin off-label therapy (1,500–2,000 mg per day) was initiated in both girls.
Presented clinical case reports demonstrate different patient complaints and clinical characteristics of type A insulin resistance syndrome. Patients with type A IR need personalized approach. High-dose metformin therapy can be used to reduce the severity of IR-associated skin symptoms such as acanthosis nigricans, papillomatosis, and polycystic ovary syndrome. Genetic diagnosis allows determining the prognosis and providing genetic counseling.

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0).
ISSN 2072-0378 (Online)









































