



Jubilee Greetings

February 12, 2026, marks the 85th birthday of Academician of the Russian Academy of Sciences Ivan Ivanovich Dedov. He serves as President of the State Research Center of the Russian Federation – Endocrinology Research Centre, Chief NonStaff Endocrinologist of the Russian Ministry of Health, Hero of Labour of the Russian Federation, and is a full holder of the Order "For Merit to the Fatherland".
Evidence Based Diabetology

OBJECTIVE. To analyze and describe existing methods for the diagnosis and treatment of diabetic neuroosteoarthropathy.
MATERIALS AND METHODS. A search and analysis of clinical trials, meta-analyses, systematic reviews and clinical guidelines on the diagnosis and treatment of Charcot neuroarthropathy was conducted. The literature search was carried out across the MEDLINE, ELibrary, PubMed, Web of Science, Google Scholar, and Clinical Key databases. The search covered a 20-year period; publications of historical significance were also included.
RESULTS. A total of 165 publications were incorporated into this review. The paper outlines key features of the clinical presentation and course of diabetic neuroosteoarthropathy, and summarizes current scientific understanding of its etiology, classification, diagnostic criteria and treatment options.
CONCLUSION. Implementation of the proposed algorithms will help to objectify the diagnosis and improve the quality of medical care provided to patients with Charcot neuroarthropathy.
Original Studies
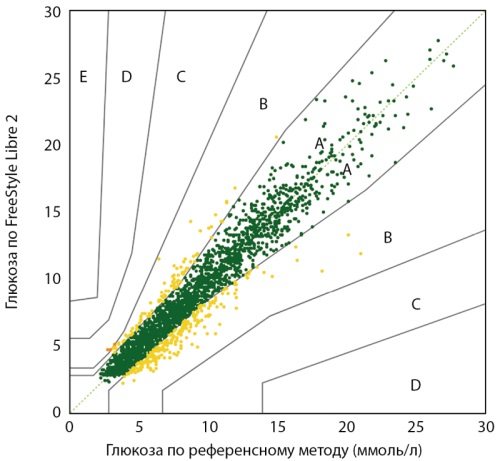
BACKGROUND. Continuous glucose monitoring (CGM) is becoming the standard of care for children with type 1 diabetes (T1D), yet data on its use in children under 4 years old remain limited. FreeStyle Libre 2 (FSL2) is approved for use from the age of 4, but there is a clinical need for use in younger age groups.
OBJECTIVE. To evaluate the accuracy and safety of the FSL2 system when used off-label in children aged 1–4 years with T1D.
MATERIALS AND METHODS. The study included 20 children with T1D (mean age 2.8±0.7 years, diabetes duration 1.2±0.8 years, HbA1c 7.1±1.4%). Participants consecutively used two FSL2 sensors over a 28-day period. Accuracy was assessed by comparing FSL2 data to reference capillary blood glucose measurements (≥6 times daily). Analyses included mean absolute relative difference (MARD), agreement rates, and distribution across zones of the Parkes consensus error grid.
RESULTS. A total of 2,554 paired measurements were analyzed. Overall MARD was 11.5% (95% CI: 10.6–12.3%). Agreement rates: 74.6% of readings were within ±15%/15 mg/dL, and 84.2% within ±20%/20 mg/dL. A total of 99.9% of readings fell within Zones A+B of the consensus error grid. MARD remained stable over the 14-day sensor wear period (11.9%, 11.1%, 11.7% in the initial, middle and final periods of use). The average sensor wear time was 285.7±95.9 hours. No serious adverse events were reported; local skin reactions were mild and resolved fully without any treatment.
CONCLUSION. FSL2 demonstrated clinically acceptable accuracy and a high safety profile in children aged 1–4 years with T1D. The findings support potential extension of FSL2 use in this age group to improve glycemic control and family quality of life.
BACKGROUND: There has been an increasing focus on the use of digital systems for remote monitoring (RM) of patient health recently.
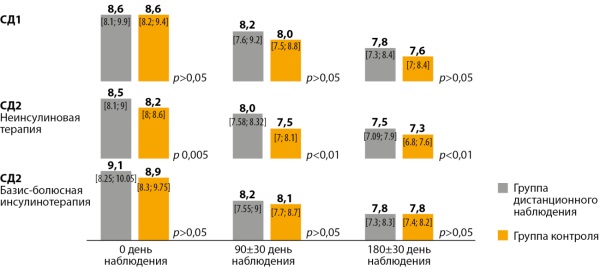
AIM: To evaluate the clinical effectiveness of the RM system in patients with type 1 and type 2 diabetes (T1D and T2D) compared to traditional outpatient care.
MATERIALS AND METHODS: a non-randomized prospective open comparative multicenter study with parallel groups was conducted in 7 regions of the Russian Federation from March to September 2024. The study included patients with T1D, T2D on non-insulin therapy, and T2D on insulin therapy. The intervention group used a glycaemia RM system, which included a glucometer with a data transmission set, a mobile application that received data from the glucometer via Bluetooth technology, and a data transmission system for the doctor. In the control group, glycemia was assessed as part of routine clinical practice (in-person visits with a self-monitoring diary).
RESULTS: A total of 1,572 patients were included in the study. After a 180-day follow-up, the overall completion rate was 48% (754 patients). The primary endpoint, HbA1c levels, decreased comparably in the RM and control groups in patients with T1DM and in both cohorts of patients with T2DM. The proportion of individuals who achieved HbA1c target values was higher in the RM group compared to the control group in patients with T1DM (26.06% vs. 10.91%, respectively, p=0.023) and T2DM on non-insulin therapy (51.5% vs. 33%, respectively, p=0.003). RM use was associated with a reduction in unscheduled medical interventions.
CONCLUSION: RM has shown clinical efficacy in increasing the proportion of patients achieving HbA1c target values in the group of patients with T1D and T2D on non-insulin antidiabetic therapy.
RELEVANCE. Type 2 diabetes mellitus (DM2) is closely related to obesity and insulin resistance (IR). Semaglutide, glucagon-like peptide-1 receptor agonist, exhibits pronounced effects on glycemic control and body weight. However, data on its effect on various surrogate IR indices in routine practice are limited.
AIM. To evaluate the effect of semaglutide (Semavic®) on metabolic control and IR in patients with DM2 and obesity who did not achieve the target values of carbohydrate metabolism on metformin monotherapy.
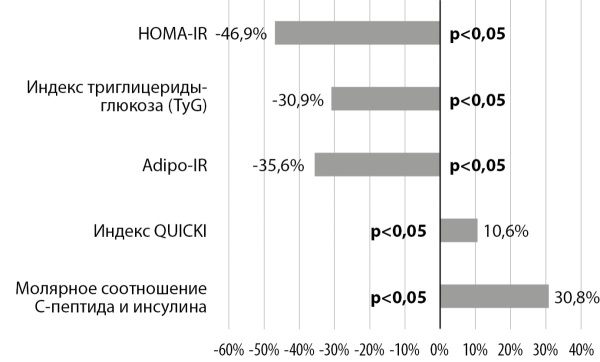
MATERIALS AND METHODS. The prospective study included 31 patients aged 40–65 years with DM2, BMI 30.0–39.9 kg/m2 and HbA1c 7.0–9.0% on metformin treatment; 28 patients completed a 24-week follow-up. Anthropometric parameters, bioimpedance body composition, HbA1c, fasting glycemia, insulin, C-peptide, free fatty acids were evaluated. HOMA-IR, QUICKI, TyG, Adipo-IR indices, C peptide/insulin molar ratio were calculated.
RESULTS. After 24 weeks of semaglutide therapy, there was a significant decrease in body weight (median -8.2% or 8.58 kg), BMI, waist circumference and fat mass as well as an improvement in carbohydrate metabolism: HbA1c had decreased from 7.63% to 6.25%, 85.7% of patients reached HbA1c <7.0%. There was a significant decrease of HOMA-IR, TyG, Adipo-IR indices, an increase of QUICKI and C peptide/insulin molar ratio indicating a decrease of IR in the liver, adipose and peripheral tissues. Adverse events were observed in a small proportion of patients and were mainly of a temporary dyspeptic nature.
CONCLUSIONS. Semaglutide in patients with DM2 and obesity in real clinical practice provides a significant reduction of body weight, improves glycemic control and leads to multicomponent reduction of IR with a favorable safety profile.
Case report

Slowly developing immune-mediated diabetes mellitus in adults combines the phenotypic and immunological characteristics of type 1 and type 2 diabetes mellitus, which often complicates the correct diagnosis and timely initiation of appropriate glucose-lowering therapy. The article presents a clinical case of a 46-year-old patient with slowly evolving immune-mediated diabetes with multiple complications, initially diagnosed as type 2 diabetes mellitus, upon hospitalization in a surgical hospital for phlegmon of the right foot. A feature of the clinical case is the complications, the severity of which did not correspond to the known duration of the disease and was due to a "hidden", long-term course. The correct diagnosis established during the diagnostic search will avoid attempts to prescribe incorrect therapy to the patient in the future, which can lead to decompensation of carbohydrate metabolism and progression of late complications. With this article, we want to draw the attention of endocrinologists and doctors of other specialties to the complexity, diversity of the clinical course of LADA diabetes and the need for differential diagnosis, a detailed collection of the disease history, as well as the importance of determining autoantibodies in the atypical course of type 2 diabetes mellitus.
Erratum
Erratum: "Rotary activity as the main electrophysiology mechanism of the persistent form of atrial fibrillation of patients with type 2 diabetes mellitus" by Irina A. Bulavina, Igor A. Khamnagadaev, Nikolay I. Tyurin, Ekaterina K. Melkozerova, Leonid A. Belousov, Irina Z. Bondarenko, Olga A. Shatskaya, Ilya L. Ilyich, Viktor Y. Kalashnikov published in Diabetes Mellitus. 2025;28(6):314-320. doi: 10.14341/DM13412.
An error occurred in the author list of the original article: Natalia G. Mokrysheva was inadvertently omitted from the author list. The correct list of authors is as follows: Irina A. Bulavina, Igor A. Khamnagadaev, Nikolay I. Tyurin, Ekaterina K. Melkozerova, Leonid A. Belousov, Irina Z. Bondarenko, Olga A. Shatskaya, Ilya L. Ilyich, Viktor Y. Kalashnikov, Natalia G. Mokrysheva. The Editorial Office regrets this error. The original version of the article has been replaced.

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License (CC BY-NC-ND 4.0).
ISSN 2072-0378 (Online)









































