




Contents
Scroll to:
https://doi.org/10.14341/DM13112
Scroll to:
BACKGROUND: Diabetes mellitus is a prevalent condition in Saudi Arabia, with approximately 20% of the adult population affected, ranking sixth highest in the world. This disease is associated with both acute and chronic complications. Among these complications, hypoglycemia is particularly dangerous and can occur during diabetes treatment. Individuals diagnosed with type 1 diabetes may experience multiple episodes of asymptomatic or symptomatic hypoglycemia per week.
AIM: To assess the frequency of hypoglycemic episodes and identify associated factors among individuals with type 1 diabetes in Unaizah City, Saudi Arabia.
MATERIALS AND METHODS: A quantitative, cross-sectional, descriptive research design was employed in April and May of 2023. A convenience sample of 280 type 1 diabetic clients living in the Qassim region of Unaizah City was selected. Participants completed an electronic structured questionnaire that collected information on sociodemographic factors and hypoglycemia-related data. Descriptive statistics and a Chi-square test were used for data analysis, utilizing SPSS version 23. Ethical considerations were strictly adhered to throughout the study.
RESULTS: The findings revealed that over two-thirds of the participants (72.1%) reported experiencing hypoglycemic episodes within the past week. Furthermore, more than one-fifth of these individuals attributed the cause of the episodes to high insulin doses (21%). Seeking medical assistance to change medications for hypoglycemia was reported by more than half of the participants (55.4%), while less than half received help from others during hypoglycemic episodes (42.9%). It was observed that adherence to diabetic medication was higher than adherence to diabetic diet and exercise regimens. Males, as well as single or divorced participants, reported a higher frequency of hypoglycemic episodes. Additionally, patients with higher levels of education and those residing in rural regions reported a higher exposure to hypoglycemic episodes.
CONCLUSION: The effective management of hypoglycemia necessitates patient education and awareness regarding its causes and symptoms. Targeted interventions are required to improve adherence to therapeutic regimens and lifestyle modifications. Furthermore, when managing hypoglycemia, it is important to consider the gender, marital status, educational level, and residence of diabetic patients.
Aldekheel S., Shahin M. Hypoglycemic episodes among type 1 diabetic patients in Unaizah, Saudi Arabia: causes, management, and associated factors. Diabetes mellitus. 2024;27(1):69-80. https://doi.org/10.14341/DM13112
Diabetes is associated with serious complications such as cardiovascular diseases, renal failure, and retinopathy [1]. Among these complications, hypoglycemia is particularly concerning. Hypoglycemia is defined as «an excessively low plasma glucose concentration (70 mg/dl) that exposes the person to possible injury» [2]. It is characterized by a decrease in plasma glucose levels that can induce symptoms such as altered mental status and/or activation of the sympathetic nervous system [3].
Hypoglycemia commonly occurs in clinical practice, with approximately 90% of insulin-receiving patients experiencing hypoglycemic episodes. The prevalence of hypoglycemia is higher in patients treated with insulin compared to those not using insulin for glycemic control [4]. Although patients and physicians often attribute symptoms like anxiety, irritability, and hunger to hypoglycemia, it is important to document the presence of low blood sugar [5].
Hypoglycemia can result from various factors such as medication changes or overdoses, infection, dietary changes, metabolic changes over time, or alterations in physical activity. In some cases, no acute cause can be identified. Other potential causes include alimentary problems, idiopathic causes, fasting, insulinoma, endocrine problems, extra pancreatic causes, hepatic disease, and bariatric surgery, among others [6]. Additionally, recognized risk factors for hypoglycemia include physical activity, advancing age, co-morbidities, lack of awareness of hypoglycemia, inappropriate diet, fasting or weight loss, alcohol consumption, duration of diabetes, and time since the initiation of insulin treatment [7].
Hypoglycemia is a significant complication of diabetes treatment, with a higher risk observed in patients with comorbidities such as vascular disease or renal failure, pregnant women, and children with type 1 diabetes. In type 2 diabetes, progressive insulin deficiency, longer disease duration, and tight glycemic control contribute to an increased risk of hypoglycemia, comparable to that seen in type 1 diabetes [8].
The symptoms of hypoglycemia can vary among individuals. Low blood sugar may present with symptoms such as lack of coordination, chills, clammy skin, and sweating. Tingling or numbness in the mouth may also occur, along with blurred vision, headache, confusion, and difficulties with everyday tasks and coordination [9]. Other potential symptoms include shaking, palpitations, perspiration, anxiety, hunger, nausea, tingling, trouble concentrating, disorientation, weakness, drowsiness, vision changes, difficulty speaking, headaches, dizziness, seizures, comas, and, in severe cases, death [10].
Hypoglycemia can be categorized as mild, moderate, or severe, depending on the severity of symptoms and whether medical attention is required or the condition resolves on its own [11]. Episodes of hypoglycemia can lead to impairment of the counter-regulatory system and the development of hypoglycemia unawareness. This, in turn, increases the risk of vascular events and other detrimental effects. Individualized glycemic control, considering patient characteristics and safety, is crucial. Recognizing risk factors for hypoglycemia, regular blood glucose monitoring, appropriate treatment regimens, and educational programs for healthcare professionals and patients with diabetes are essential for maintaining good glycemic control, minimizing the risk of hypoglycemia, and preventing long-term complications [12].
The mainstay of therapy for hypoglycemia is glucose. Other medications may be administered based on the underlying cause or accompanying symptoms. Treatment options for hypoglycemia include glucose supplements (e.g., dextrose), glucose-elevating agents (e.g., glucagon, intranasal glucagon), inhibitors of insulin secretion (e.g., diazoxide, octreotide), and antineoplastic agents (e.g., streptozocin) [6]. Additional therapies include dietary interventions (frequent meals/snacks, especially at night, with complex carbohydrates), intravenous glucose infusion, and intravenous octreotide [11]. Prompt treatment is crucial to prevent severe hypoglycemia, which can lead to coma or death [13].
Hypoglycemia imposes a substantial financial burden on patients, the healthcare system, and society at large. Although patients with well-controlled type 1 diabetes may experience multiple episodes of asymptomatic hypoglycemia and approximately two episodes of symptomatic hypoglycemia per week, those with type 2 diabetes are less likely to encounter hypoglycemic events [14]. Prevention is widely recognized as the key factor in managing hypoglycemia.
Given the high prevalence and adverse impact of hypoglycemia on diabetic patients, as well as the limited number of studies conducted on hypoglycemic episodes among type 1 diabetic patients in Saudi Arabia [15], further research on this topic is needed, particularly in Unaizah City. To the best of our knowledge, no study has been conducted on this subject in Unaizah City, located in the Qassim region of Saudi Arabia. Therefore, this research aimed to investigate the incidence of hypoglycemia, its risk factors, clinical manifestations, management behaviors, and associated factors among type 1 diabetic patients in Unaizah City, Saudi Arabia.
The study aimed to assess the incidence of hypoglycemic episodes, its risk factors, clinical manifestations, management behaviors, and associated factors among type 1 diabetic patients in Unaizah City, Saudi Arabia.
The study had the following objectives:
Place of the research. The study was conducted in Unaizah City, located in the Qassim region of Saudi Arabia.
Period of the research. The data collection stage of the research extended over a two-month period (April and May 2023).
The target population for this study comprised all individuals with type 1 diabetes residing in Unaizah City. The following inclusion criteria were used to select the study sample:
Inclusion criteria
Type 1 diabetic individuals.
Age 18 or older.
Residing in Unaizah City.
Any nationality.
Able to read and write.
Willing to participate in the study.
According to the Albassam Diabetic Center in King Saud Hospital, which is the only specialized unit for diabetic care in Unaizah City, there were approximately 1,000 registered cases of type 1 diabetes at the time of data collection. Using power analysis to calculate the required sample size from the target population, it was determined that a minimum sample size of 278 cases was needed to achieve a confidence level of 95% (Figure 1) [16]. However, responses were obtained from 280 type 1 diabetic individuals from Unaizah City.
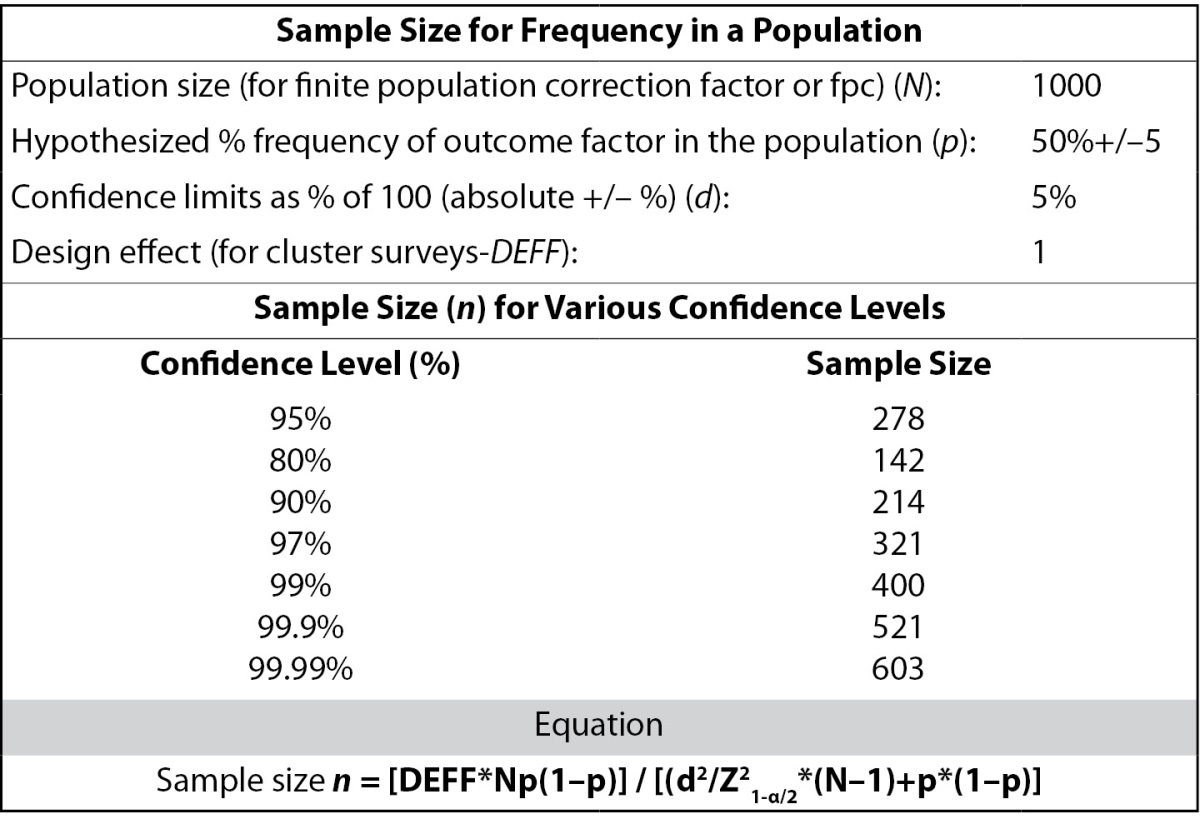
Figure 1. Sample size calculation using power analysis.
Convenience sampling was used to recruit the sample. Convenience sampling is preferred over random sampling in situations where data needs to be collected quickly, is cost-effective, and is readily available, with minimal procedural requirements [17].
A quantitative, cross-sectional, and descriptive design was employed for this study. Data was collected from participants at a specific point in time without any follow-up. This research design is suitable for conducting surveys and gathering data from a large number of participants within a short timeframe [18].
Research Instrument.
A structured questionnaire was adopted from a previous study conducted by Elshebiny, Alali [14] to assess the incidence of hypoglycemia and its risk factors among diabetic individuals in the Eastern Province of Saudi Arabia. This validated tool had been previously used by expert researchers in the same language and study setting, Saudi Arabia, thus ensuring its validity and reliability. Formal approval was obtained from the original authors to utilize their data collection tool for the current study [14]. The questionnaire consisted of two parts.
Part 1 — Demographic Factors: This section included questions about participants’ age, gender, nationality, city, place of residence, and level of education.
Part 2 — Diabetic Datasheet: This section included close-ended questions about diabetic history, duration, medications, associated diseases, hypoglycemic episodes, causes of hypoglycemia, blood glucose levels during hypoglycemia, symptoms of hypoglycemia, timing of episodes, treatment used, and adherence to the therapeutic regimen [14].
The content validity of the questionnaire was established by seeking the opinions of three experts in diabetic care, medical, and critical care nursing. Test-retest reliability was assessed through a pilot study involving 10 clients, resulting in a Cronbach’s alpha coefficient of 0.782, indicating good reliability. The results of the pilot study were not included in the study findings.
Data Collection Procedures.
Data collection was conducted using a convenience sampling technique by distributing an electronic questionnaire to most of the clients registered at the Albassam Diabetic Center as type 1 diabetic individuals, where they received their follow-up care. The questionnaire was sent through various social media platforms, including WhatsApp, SMS, Messenger, and other technologies. The cover page of the questionnaire included clear instructions about the study purpose, methods and ethical considerations, and the importance of filling out the questionnaire personally by the patient himself/herself. Only participants who met the inclusion criteria were invited to complete the questionnaire. The questionnaire was distributed multiple times to the participants over a two-month period (April and May 2023) to achieve the desired number of responses.
Following data collection, the collected data was analyzed using the Statistical Package for Social Sciences software (SPSS) Version 23 [19]. Descriptive statistics, such as mean and standard deviation for continuous variables, and numbers and percentages for categorical variables, were used for analysis. The results were presented in tables and graphs. Additionally, the Chi-square test was employed to examine the association between hypoglycemia episodes and participants’ sociodemographic characteristics.
Ethical approval for data collection was obtained from the Research Ethics Committee of the Faculty of Nursing at Hail University (Ethics Committee decision No. H-2023-184 on 3/4/2023). A research facilitation letter was also obtained from the Faculty of Nursing to the Albassam Diabetic Center at King Saud Hospital. Human rights were protected by ensuring voluntary participation and obtaining participants’ approval or consent to complete the survey.
Participant identities were protected by assigning numbers to their responses and not requesting any personally identifying information in the questionnaire. Anonymity, confidentiality, and autonomy were maintained to ensure participants’ privacy and freedom to participate in the study. The collected data was securely stored on the researcher’s personal computer in an encrypted file, protected by a password, to ensure data safety and prevent any potential data breaches. All ethical considerations regarding scientific research involving human subjects were strictly adhered to in accordance with the Declaration of Helsinki [20].
The current study aimed to assess hypoglycemic episodes and their associated factors among individuals with type 1 diabetes in Unaizah City. The study results were presented through tables and figures, which depicted the sociodemographic characteristics of the participants, their diabetic profile, and information about hypoglycemic episodes.
Table 1 provides sociodemographic data for 280 participants residing in Unaizah City, Saudi Arabia. The majority of participants were between 18 and 30 years old (51.1%), and most of them were female (63.2%). The participants’ ages ranged from 19 to 72 years, with a mean age of 32.71 years and a standard deviation of 13.44. Nearly all participants were Saudi nationals (98.2%) and lived in urban regions (90%). Approximately half of the participants were single (48.2%) or married (47.9%), and the majority had attained a university-level education (47.1%).
Table 1. Sociodemographic data of the participants (N=280)
Sociodemographic data | n | % | |
Age | From 18 to 30 years | 143 | 51.1% |
From 31 to 40 years | 74 | 26.4% | |
From 41 to 50 years | 23 | 8.2% | |
From 51 to 60 years | 29 | 10.4% | |
More than 60 years | 11 | 3.9% | |
Mean ± SD= 32.71±13.44 | |||
Gender | Female | 177 | 63.2% |
Male | 103 | 36.8% | |
Nationality | Saudi | 275 | 98.2% |
Non-Saudi | 5 | 1.8% | |
Region | Rural region | 28 | 10.0% |
Urban region | 252 | 90.0% | |
Marital status | Married | 134 | 47.9% |
Single | 135 | 48.2% | |
Divorced | 11 | 3.9% | |
Educational level | Only read and write | 3 | 1.1% |
Primary education | 12 | 4.3% | |
Intermediate education | 41 | 14.6% | |
Secondary education | 80 | 28.6% | |
University education | 132 | 47.1% | |
Postgraduate education | 12 | 4.3% | |
Table 2 presents the medical history and chronic diseases of the 280 participants with type 1 diabetes as per the reported data in the questionnaires. Regarding the duration of diabetes, 23.2% of participants had been living with the disease for 1 to 5 years, while 24.3% did not remember. In terms of medication, 68% of participants used fast-acting and long-acting insulin, 13% used Mixtard insulin, and 19% used insulin pumps. As for chronic diseases, 48.57% of participants reported having no chronic diseases, while 30.71% had hypertension, 17.86% had hypothyroidism, 14.29% had heart disease, 12.14% had kidney disease, and 7.14% had asthma.
Table 2. Medical history of the participants (N=280)
Item | n | % | |
Duration of type-1 diabetes | 1 to 5 years | 65 | 23.20% |
6 to 10 years | 61 | 21.80% | |
11 to 15 years old | 26 | 9.30% | |
16 years or older | 60 | 21.40% | |
I do not remember | 68 | 24.30% | |
The therapeutic regimen used | Fast and long-acting insulin | 189 | 68% |
Mixtard insulin | 37 | 13% | |
Insulin Pump | 54 | 19% | |
Having chronic diseases | Hypertension | 86 | 30.71% |
Heart disease | 40 | 14.29% | |
Kidney disease | 34 | 12.14% | |
Asthma | 20 | 7.14% | |
Hypothyroidism | 50 | 17.86% | |
No chronic diseases | 136 | 48.57% | |
Table 3 provides data on the participants’ hypoglycemia history. Among the participants, 27.9% reported no recent hypoglycemic episodes, while 72.1% reported experiencing hypoglycemia in the last week, and among them, 15% had at least three episodes of hypoglycemia in the last week. The most common cause of hypoglycemia was taking a high dose of insulin (21%), followed by eating after a long period of insulin use (18%). The majority of participants (62.5%) used both blood glucose level measurements and symptoms to identify hypoglycemic episodes.
Table 3. Hypoglycemia history of the participants (N=280)
Item | n | % | |
During the last week, the number of hypoglycemic episodes | None | 78 | 27.9% |
Once | 44 | 15.7% | |
Twice | 32 | 11.4% | |
3 times | 31 | 11.1% | |
More than 3 times | 42 | 15.0% | |
I do not remember the number | 53 | 18.9% | |
Cause of hypoglycemic episodes | Inappropriate diet (ex: extreme diet to lose weight) | 28 | 10.0% |
Loss of appetite | 21 | 8.0% | |
Missing a meal | 30 | 11.0% | |
Eating after a long period of insulin use | 50 | 18.0% | |
Sports and hard exercise | 29 | 10.0% | |
Lack of knowledge about hypoglycemia | 18 | 6.0% | |
No adherence to medications (using medications at random times) | 21 | 8.0% | |
Taking high doses of insulin | 60 | 21.0% | |
Not measuring blood glucose regularly | 30 | 11.0% | |
Increase the dose without consulting a doctor. | 11 | 4.0% | |
Due to other chronic diseases | 7 | 3.0% | |
Other | 11 | 4.0% | |
The method used for hypoglycemia diagnosis | By measuring blood glucose level | 37 | 13.2% |
Symptoms of hypoglycemia | 68 | 24.3% | |
Both | 175 | 62.5% | |
Blood glucose level for the last hypoglycemic episode | less than 40 | 25 | 8.9% |
From 40 to 49 | 29 | 10.4% | |
From 50 to 59 | 90 | 32.1% | |
From 60 to 69 | 73 | 26.1% | |
I did not do the checkup | 36 | 12.9% | |
I do not remember | 27 | 9.6% | |
Common symptoms of hypoglycemic episode | Sweating | 63 | 23.0% |
Extreme hunger | 41 | 15.0% | |
Feeling stressed and anxious | 37 | 13.0% | |
Shiver (tremor) | 67 | 24.0% | |
Paresthesia of the limbs | 17 | 6.0% | |
Heart palpitations | 39 | 14.0% | |
Nausea | 10 | 4.0% | |
Headache | 25 | 9.0% | |
Dizziness | 46 | 16.0% | |
Imbalance | 31 | 11.0% | |
Blurry eyes | 33 | 12.0% | |
Exhaustion | 28 | 10.0% | |
Mood swings | 27 | 10.0% | |
Difficulty concentrating | 37 | 13.0% | |
Difficulty speaking | 23 | 8.0% | |
Spasm | 4 | 1.0% | |
Coma | 2 | 1.0% | |
I did not suffer from any symptoms | 9 | 3.0% | |
Time of hypoglycemic episode occurrence | Afternoon | 38 | 13.6% |
At night | 44 | 15.7% | |
Different times | 184 | 65.7% | |
In the morning | 14 | 5.0% | |
For about one-third of the participants (32.10%), the blood glucose level during the last hypoglycemia episode was reported to be 50 to 59 mg/dl. The most frequently reported symptoms during hypoglycemic episodes were shivering/tremors (24%) and sweating (23%), and the episodes occurred at different times of the day for the majority of participants (65.7%).
Table 4 delineates the strategies employed by participants in managing hypoglycemic episodes. Among the 280 participants, 2.1% opted for glucagon injection, 10% sought medical care or visited an emergency center, 55.4% resorted to the consumption of food, and 32.5% adhered to the 15-15 Rule for addressing the majority of hypoglycemic episodes. When queried about seeking assistance from others in managing hypoglycemia, 42.9% of participants affirmed, while 57.1% negated receiving external help. Regarding the reported alterations in diabetic medication for hypoglycemia management in general, 37.5% of participants endeavored to identify the underlying cause of hypoglycemia, 28.9% reduced their hypoglycemic medications or insulin dosage, 4.6% maintained the same medication dosage, and 28.9% reported abstaining from medication usage.
Table 4. Hypoglycemic episodes management
and compliance with diabetic therapeutic regimen (N=280)
Item | n | % | ||
Hypoglycemic Episodes Management | Treatment used for hypoglycemic episodes | Glucagon injection | 6 | 2.10% |
Going to a medical care or emergency center | 28 | 10.00% | ||
Using food | 155 | 55.40% | ||
Using the 15-15 Rule | 91 | 32.50% | ||
Have someone else helped you during hypoglycemia treatment | Yes | 120 | 42.90% | |
No | 160 | 57.10% | ||
Changes in medications to treat hypoglycemic episodes | Find out the reason for hypoglycemia | 105 | 37.50% | |
Reduce the dose of hypoglycemic medications | 81 | 28.90% | ||
Used the same dose of hypoglycemic medications | 13 | 4.60% | ||
I did not use medication | 81 | 28.90% | ||
Consult a physician, about the procedure followed to treat episodes of hypoglycemia | Changed diabetic medications | 30 | 10.70% | |
Reduced the dose of diabetic drugs | 93 | 33.20% | ||
Maintained the same drugs | 32 | 11.40% | ||
I didn’t consult a physician | 125 | 44.60% | ||
Diabetes Management Regimen | Diabetic management, compliance with diabetic medications regularly | A little | 42 | 15.00% |
Most days | 43 | 15.40% | ||
Everyday | 195 | 69.60% | ||
Diabetic management, compliance to diabetic diet | A little | 144 | 51.40% | |
Most days | 97 | 34.60% | ||
Everyday | 39 | 13.90% | ||
Diabetic management, compliance with exercising regularly | A little | 136 | 48.60% | |
Most days | 105 | 37.50% | ||
Everyday | 39 | 13.90% | ||
In terms of consulting physicians for hypoglycemia treatment and subsequent interventions, 10.7% of participants experienced changes in their prescribed medication, 33.2% witnessed a reduction in their medication dosage, 11.4% persisted with the same medication regimen, while 44.6% indicated a lack of consultation with physicians when faced with hypoglycemia.
The table also provides information regarding the participants’ adherence to their diabetic therapeutic regimen. Out of the 280 participants, 69.6% reported being fully committed to using diabetic medications every day, while 15.4% reported being mostly committed to using them, and 15.0% reported being only partially committed. Regarding adherence to the diabetic diet, 51.4% of the participants reported being only partially committed, 34.6% reported being mostly committed, and 13.9% reported being fully committed. Concerning regular exercise, 48.6% of the participants reported being only partially committed, 37.5% reported being mostly committed, and 13.9% reported being fully committed. Overall, most participants reported being fully committed to using diabetic medications daily, while adherence to the diabetic diet and exercise were reported to be lower.
Utilizing chi-square statistics to evaluate the association between the incidence of hypoglycemia and sociodemographic characteristics among participants, a p-value of less than 0.001 was obtained for participants’ gender, living region, marital status, and educational level. This underscores a highly significant association between the occurrence of hypoglycemic episodes and participants’ gender, living area, marital status, and educational level.
Upon examination of Figure 2, a conspicuous observation emerges—nearly three-fourths (79%) of male participants experienced hypoglycemia, whereas only 66% of female participants encountered such episodes. This discrepancy highlights a significantly higher percentage of hypoglycemic episodes among male participants in comparison to their female counterparts.
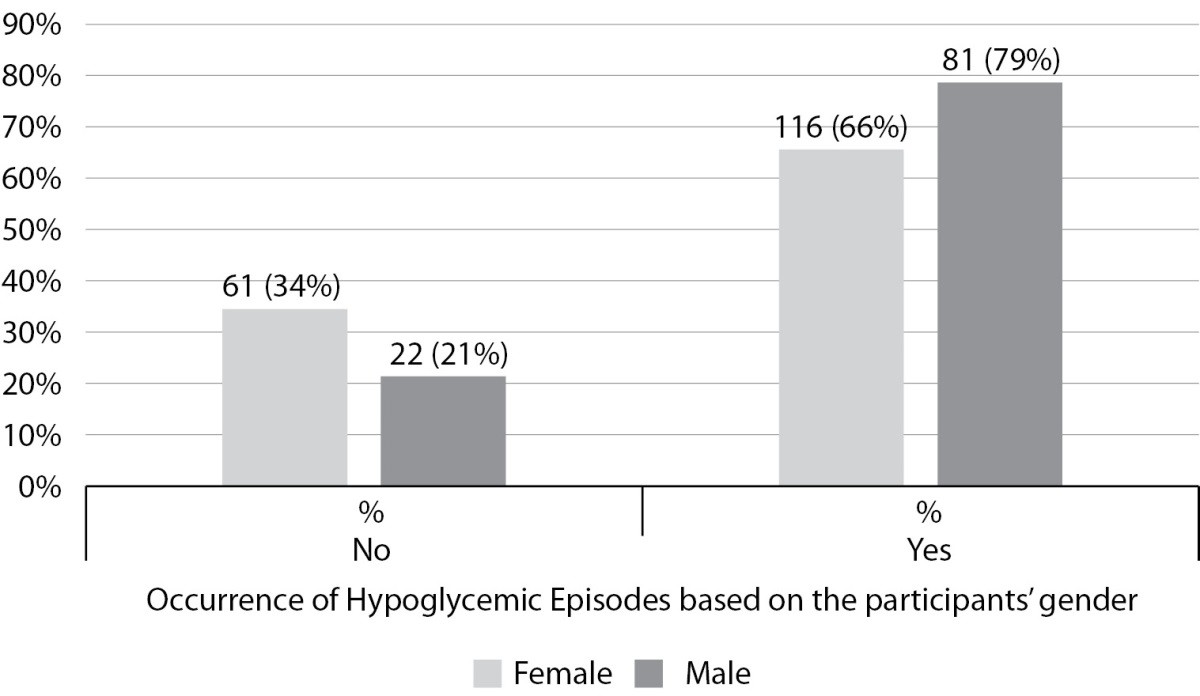
Figure 2. Relationship between experienced hypoglycemia episodes
among the participants and their gender (N=280)
Concerning participants’ educational levels, a discernible pattern emerges in the context of hypoglycemia experiences. Among non-educated participants with basic literacy skills, none reported experiencing hypoglycemia. Similarly, 80% of participants with primary education did not encounter hypoglycemia. However, among participants with intermediate education, 59% reported experiencing hypoglycemia, and for those with secondary education, the percentage increased to 76%. Among participants with a university education, 68% reported hypoglycemia, with the percentage rising to 83% among those with postgraduate education.
Figure 3 distinctly illustrates a trend where a higher percentage of participants with elevated educational levels (secondary education, university education, and postgraduate education) reported experiencing hypoglycemia compared to those with lower educational levels (non-educated individuals, participants with primary education, or intermediate education).
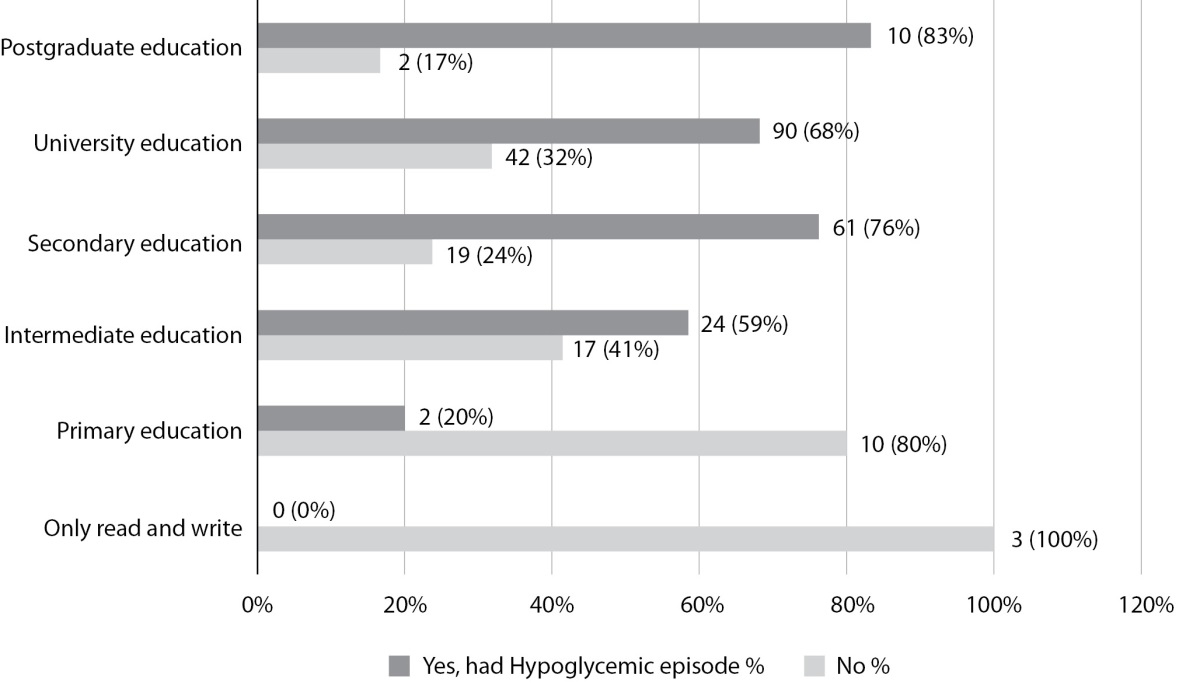
Figure 3. Experience of hypoglycemic episodes to participants’ educational level (N=280)
Table 5 presents information concerning the occurrence of hypoglycemic episodes based on participants’ living place and marital status. The chi-square test results demonstrate a significant association between the occurrence of hypoglycemia and both the participants’ living region and marital status (Asymp. Sig. = 0.000).
Table 5. Relationship between experienced hypoglycemia episodes
among the participants and their living region and marital status (N=280)
| Experienced hypoglycemia episode | Total | Chi-Square | Asymp. Sig. | ||||
No | Yes | |||||||
n | % | n | % | n | ||||
Region | Urban | 81 | 47% | 171 | 68% | 252 | 179.200a | .000** |
Rural | 2 | 8% | 26 | 93% | 28 | |||
Total | 83 | 42% | 197 | 70% | 280 | |||
Marital status | Single | 29 | 21.5% | 106 | 78.5% | 135 | 108.950b | .000** |
Married | 51 | 38% | 83 | 62% | 134 | |||
Divorced | 3 | 27.3% | 8 | 72.7% | 11 | |||
Total | 83 | 30 | 197 | 70% | 280 | |||
** Significant at <0.01
Among participants residing in rural regions, a staggering 93% reported experiencing hypoglycemia, whereas only 68% of participants living in urban areas encountered such episodes. Regarding marital status, 78.5% of single participants experienced hypoglycemia, with a slightly lower percentage of 72.7% among divorced participants. Interestingly, among married participants, the percentage dropped further to 62%. The table clearly indicates a significantly lower proportion of married participants experiencing hypoglycemic episodes compared to single and divorced participants.
The findings of the present study contribute valuable insights into hypoglycemic episodes and their associated factors among individuals with type 1 diabetes in Unaizah City. Concerning insulin regimens and the prevalence of chronic diseases among type 1 diabetic clients, the fact that 68% of participants utilized fast and long-acting insulin suggests the widespread adoption of this insulin regimen in the type 1 diabetic population. This observation aligns with prior research indicating the necessity of fast-acting insulin for postprandial glucose control and long-acting insulin for basal glucose control [21]. It is essential to emphasize, however, that the optimal insulin regimen may vary based on individual patient characteristics and needs.
The noteworthy usage of insulin pumps by 19% of participants underscores the significance of this alternative to multiple daily injections in the selected patients. Research has demonstrated that insulin pump therapy can enhance glycemic control, improve quality of life, and lead to reduced HbA1c levels and fewer hypoglycemic episodes [22]. It is imperative to acknowledge that insulin pump therapy may not be universally suitable, necessitating close monitoring and adequate training for safe and effective use.
Regarding the prevalence of chronic diseases among type 1 diabetic patients, the findings indicate that hypertension is the predominant comorbidity, affecting 30.71% of participants. This aligns with existing research highlighting the heightened risk of hypertension in individuals with diabetes, attributed to factors such as insulin resistance, obesity, and dyslipidemia [23]. Hypertension further complicates diabetes management and elevates the risk of cardiovascular complications.
In the current study, the identification of a high insulin dose as the most common cause of hypoglycemia resonates with previous research. While insulin is integral to diabetes treatment, improper dosing, whether excessive or inadequately balanced with food intake and physical activity, can lead to hypoglycemia. Existing literature emphasizes the role of insulin dosing education and self-management in preventing hypoglycemic episodes [24].
The utilization of both blood glucose level measurements and symptom awareness by the majority of participants for identifying hypoglycemic episodes constitutes a significant finding. This implies that patients actively monitor their blood glucose levels and possess awareness of hypoglycemia symptoms, a crucial aspect in the early detection and prompt management of such episodes. Prior research has underscored that frequent blood glucose monitoring can mitigate the risk of hypoglycemia and enhance glycemic control in diabetic patients [25].
Among the reported symptoms during hypoglycemic episodes, sweating (23%) and shivering/tremor (24%) emerged as the most prevalent. This aligns with earlier research identifying sweating, shakiness, and palpitations as common manifestations of hypoglycemia [14]. It is noteworthy that hypoglycemia symptoms may vary among individuals and may not always be apparent, particularly in patients with recurrent episodes.
The occurrence of hypoglycemic episodes at different times of the day for a majority of participants, as evidenced in the present study, emphasizes the unpredictable nature of hypoglycemia and its potential impact on daily activities and quality of life. Research has indicated that recurrent hypoglycemia can lead to impaired cognitive function, reduced quality of life, and increased healthcare costs [26].
Regarding the strategies adopted by diabetic patients to address hypoglycemia, the majority of participants sought to ascertain the cause before initiating treatment. This aligns with prior research emphasizing the importance of identifying the cause of hypoglycemia to prevent recurrence and effectively manage it in the future [27]. This underscores the significance of patient education and awareness regarding potential causes such as insulin dosing errors, delayed or missed meals, and physical hyperactivity.
The finding that more than one-fourth of participants in the current study reduced their medication dose to manage hypoglycemia is consistent with previous research. Adjusting the dose of glucose-lowering medication is a common strategy, particularly in cases of medication dosing errors [28]. However, it is crucial to recognize that reducing medication doses may lead to hyperglycemia with negative health consequences. Therefore, patients should consult their healthcare providers before making any adjustments to their medication regimens.
The outcome of the current study, wherein the majority of participants reported consistent adherence to daily diabetic medications, is encouraging. Medication adherence stands as a pivotal element in diabetes management. Previous research has indicated that suboptimal medication adherence can lead to inadequate glycemic control, elevated healthcare costs, and an augmented risk of diabetes-related complications [29]. Hence, the high reported adherence to medication usage in this study is a positive indication, suggesting that participants recognize the significance of medication adherence and are dedicated to effectively managing their diabetes.
Conversely, the study revealed lower adherence to diabetic diet and regular exercise. Complying with lifestyle modifications, including dietary and exercise regimens, can prove challenging for many patients. Factors such as lack of motivation, insufficient social support, and limited knowledge about healthy lifestyle practices can contribute to this diminished adherence. Prior research has demonstrated that interventions such as education, goal setting, and social support can enhance adherence to lifestyle modifications among diabetic patients [30].
In this study, nearly three-fourths of male participants reported experiencing hypoglycemia, whereas a significantly lower proportion of female participants reported similar episodes. A recent investigation by Sarteau, Kahkoska [31] has also identified a higher prevalence of hypoglycemia in males with type 1 diabetes compared to females. Nevertheless, the reasons for this gender disparity remain unclear and may stem from diverse factors such as variations in insulin sensitivity, sex hormones, or behavioral aspects. Studies have posited that males may face an elevated risk of hypoglycemia due to heightened insulin requirements, increased physical activity, and less frequent monitoring of blood glucose levels [31].
The finding that a higher percentage of participants with advanced educational levels have experienced hypoglycemia in comparison to those with lower educational levels is intriguing. Several explanations may be considered to comprehend this phenomenon. One plausible explanation is that individuals with higher educational levels may be engaged in more demanding and stressful occupations, thereby increasing their susceptibility to hypoglycemia. Research has illustrated the impact of stress on blood sugar levels, and those with more demanding jobs may encounter heightened stress levels routinely [32]. Additionally, individuals with higher educational levels may have greater access to unhealthy food options, such as fast food or highly processed snacks, potentially heightening their risk of developing hypoglycemia.
An alternative explanation for the higher incidence of hypoglycemia among individuals with higher educational levels could be associated with their older age, exposing them to more age-related risks. Moreover, individuals with advanced education may be more inclined to adopt health-seeking behaviors, such as regular blood sugar monitoring and strict adherence to prescribed diet and medication regimens. This heightened awareness of their health may increase the probability of testing and detecting hypoglycemic episodes promptly.
The observation that a greater percentage of participants residing in rural areas have experienced hypoglycemia compared to their urban counterparts implies potential disparities in healthcare access and resources between these settings. Rural regions often face a shortage of healthcare providers and resources in comparison to urban areas, potentially resulting in reduced diabetic follow-up and delayed diagnosis and treatment of hypoglycemia, thereby increasing its severity. Additionally, limited access to healthy food options in rural areas may contribute to the development of hypoglycemia.
The identification that a higher percentage of single and divorced participants have experienced hypoglycemia compared to their married counterparts may be elucidated by differences in lifestyle factors. Single or divorced individuals may be more prone to engaging in risky behaviors, such as skipping meals or consuming unhealthy food, elevating their risk of hypoglycemia. Additionally, they may experience less social and family support, impacting their ability to effectively manage diabetes and prevent hypoglycemia. These findings diverge from a recent Saudi study that found no significant difference in hypoglycemia based on gender, educational level, or geographic distribution of diabetic patients [33]. Consequently, further research is necessary to corroborate these findings and explore the underlying factors influencing the relationship between rural and urban living and marital status with the incidence of hypoglycemic episodes among type 1 diabetic patients.
Limitations of the current research include the utilization of a convenience sampling technique from a single geographical area in Saudi Arabia, posing a primary threat to the study’s generalizability. Additionally, it is crucial to acknowledge that the findings are reliant on self-reports from participants, introducing the potential for recall bias and limiting the generalizability to the broader diabetic population. Consequently, further studies employing objective measures of hypoglycemia are imperative to validate these findings.
In future research, it is recommended to conduct more robust studies using a comparative research design taking more in-depth information from type-I diabetic patients around Saudi Arabia and considering a larger sample size.
In conclusion, healthcare providers must tailor treatment plans to meet the unique needs of each diabetic patient, taking into account the causes of hypoglycemic episodes and coexisting conditions. The majority of participants, who utilized both blood glucose level measurements and symptoms to identify hypoglycemic episodes, underscore the vital role of patient education and awareness. Proper insulin dosing education, meal planning, and self-monitoring of blood glucose levels are crucial in preventing hypoglycemia.
This study emphasizes the imperative for enhanced patient education and guidance from healthcare providers to improve the management of potential hypoglycemic episodes. Healthcare providers should educate patients on identifying the causes of hypoglycemia, adjusting medication doses, adhering to a diabetic diet, and monitoring blood glucose levels. Promoting patient empowerment and active participation in hypoglycemia management is paramount.
The lower reported adherence to the diabetic diet and exercise underscores the necessity for targeted interventions to enhance lifestyle modifications. Healthcare providers should recognize the association between diabetic patients’ gender, residential location, educational level, and marital status with hypoglycemic episodes. Efforts to improve access to healthy food options and promote healthy lifestyle behaviors can help reduce the incidence of hypoglycemia across all populations, irrespective of geographical location or marital status.
Healthcare providers should consider the potential impact of hypoglycemia on patient outcomes, including cognitive function and quality of life. Effective management strategies should be implemented to prevent or minimize hypoglycemic episodes, involving adjustments to medication regimens, promotion of regular meal planning and physical activity, and comprehensive patient education on hypoglycemia prevention and management.
Further research is necessary to identify specific barriers to adherence in this population and develop interventions accordingly. Moreover, more research is needed to enhance the understanding of the causes and management of hypoglycemia, especially in high-risk populations. Investigating the reasons behind differences in hypoglycemia prevalence and risk factors related to gender, marital status, education, and residential area is crucial. Detailed studies are needed to explore these differences and provide insights into tailored management approaches.
The impact of social support on diabetes management should be considered, with patients encouraged to build strong support networks. Healthcare providers should also be mindful of potential disparities in healthcare access and resources between rural and urban areas. Striving for equitable care for patients in all settings is essential, ensuring that appropriate resources and support are available to address hypoglycemia effectively, especially for type 1 diabetics.
The source of financing. No funding was received by the researchers for this research.
Conflicts of interests. The researchers declare that no conflicts of interest exist for this research work.
Participation of authors. Sara Khalifah Saleh Aldekheel- contribution to data collection, drafted the paper, and reviewed the manuscript; Mahmoud Abdel Hameed Shahin-contribution to the concept or study design, performed the statistical analyses, and edited the manuscript.
Both authors provided input regarding the manuscript and approved the final version of the article before the publication and expressed their consent to be responsible for all aspects of the work, which implies proper investigation and resolving of issues related to the accuracy or integrity of any part of the work.
Acknowledgments. We express sincere gratitude to the diabetic patients in Unaizah City who participated in this study by filling out the questionnaire. Their valuable input and willingness to share their experiences and insights greatly contributed to the research. We also extend heartfelt appreciation to the Albassam Diabetic Center at King Saud Hospital for their cooperation and support throughout the study.
1. Abdelbagi, O., Musa, I. R., Musa, S. M., ALtigani, S. A., & Adam, I. (2021). Prevalence and associated factors of hypertension among adults with diabetes mellitus in northern Sudan: a cross-sectional study. BMC cardiovascular disorders, 21, 1-7.
2. Agrawal, S., Makuch, S., Drozdz, M., Dudzik, T., Domanski, I., Poreba, R., & Mazur, G. (2022). The Impact of Hypoglycemia on Patients with Diabetes Mellitus: A Cross-Sectional Analysis. Journal of Clinical Medicine, 11(3), 626. https://doi.org/10.3390/jcm11030626
3. Alagiakrishnan, K., & Mereu, L. (2010). Approach to managing hypoglycemia in elderly patients with diabetes. Postgraduate medicine, 122(3), 129-137. https://doi.org/10.3810/pgm.2010.05.2150
4. AlTowayan, A., Alharbi, S., Aldehami, M., Albahli, R., Alnafessah, S., Alharbi, A. M., & Alharbi, S. M. (2023). Awareness Level of Hypoglycemia Among Diabetes Mellitus Type 2 Patients in Al Qassim Region. Cureus, 15(2).
5. Bonds, D. E., Kurashige, E. M., Bergenstal, R., Brillon, D., Domanski, M., Felicetta, J. V., . . . Group, A. S. (2007). Severe hypoglycemia monitoring and risk management procedures in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial. The American journal of cardiology, 99(12A), 80i-89i. https://doi.org/10.1016/j.amjcard.2007.03.026
6. Chaudhury, A., Duvoor, C., Reddy Dendi, V. S., Kraleti, S., Chada, A., Ravilla, R., . . . Mirza, W. (2017). Clinical Review of Antidiabetic Drugs: Implications for Type 2 Diabetes Mellitus Management. Frontiers in endocrinology, 8, 6. https://doi.org/10.3389/fendo.2017.00006
7. Dean, A., Sullivan, K., & Soe, M. (2013, 2013/04/06). OpenEpi: Open Source Epidemiologic Statistics for Public Health, Version. Retrieved 15 Mar, 2023 from https://www.openepi.com/Menu/OE_Menu.htm
8. Deedwania, P. (2018). Dangers of Hypoglycemia in Cardiac Patients With Diabetes: Time to Switch to Safer, Newer Drugs. J Am Coll Cardiol, 72(15), 1787-1789. https://doi.org/10.1016/j.jacc.2018.08.2138
9. Diabetes Canada Clinical Practice Guidelines Expert, C., Yale, J. F., Paty, B., & Senior, P. A. (2018). Hypoglycemia. Can J Diabetes, 42 Suppl 1(42), S104-S108. https://doi.org/10.1016/j.jcjd.2017.10.010
10. Elshebiny, A., Alali, H., Alamer, Z., Alsultan, Y., Alkhalaf, H., Alkishi, A., & Alsuwaylih, M. (2021). The incidence of hypoglycemia and its risk factors among diabetic patients in the Eastern Province of Saudi Arabia. International Journal of Medicine in Developing Countries, 5(2), 614-621. https://doi.org/10.24911/ijmdc.51-1609148506
11.
12. Etikan, I., Musa, S. A., & Alkassim, R. S. (2016). Comparison of convenience sampling and purposive sampling. American journal of theoretical and applied statistics, 5(1), 1-4.
13. Geller, A. I., Shehab, N., Lovegrove, M. C., Kegler, S. R., Weidenbach, K. N., Ryan, G. J., & Budnitz, D. S. (2014). National estimates of insulin-related hypoglycemia and errors leading to emergency department visits and hospitalizations. JAMA internal medicine, 174(5), 678-686. https://doi.org/10.1001/jamainternmed.2014.136
14. Gonzalez, C., Monti, C., Pinzon, A., Monsanto, H., Ejzykowicz, F., & Group, A. R. (2018). Prevalence of hypoglycemia among a sample of sulfonylurea-treated patients with Type 2 diabetes mellitus in Argentina: The real-life effectiveness and care patterns of diabetes management (RECAP-DM) study. Endocrinología, Diabetes y Nutrición, 65(10), 592-602.
15. Hamdy, O. (2021). Hypoglycemia. Medscape. Retrieved 10 Oct, 2023 from https://emedicine.medscape.com/article/122122-overview?icd=login_success_email_match_norm
16. IBM Corp. (2015). IBM SPSS Statistics for Windows. In (Version 23.0) Armonk, NY: IBM Corp. https://www.ibm.com/support/pages/how-cite-ibm-spss-statistics-or-earlier-versions-spss
17. International Diabetes Federation. (2021). Diabetes facts & figures. International Diabetes Federation. Retrieved 22 Oct, 2023 from https://idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html#:~:text=The%20IDF%20Diabetes%20Atlas%20Tenth,and%20783%20million%20by%202045.
18. Kahsay, H., Fantahun, B., Nedi, T., & Demoz, G. T. (2019). Evaluation of Hypoglycemia and Associated Factors among Patients with Type 1 Diabetes on Follow-Up Care at St. Paul's Hospital Millennium Medical College, Addis Ababa, Ethiopia. J Diabetes Res, 2019(9037374), 9037374. https://doi.org/10.1155/2019/9037374
19. Kallem, V. R., Pandita, A., & Gupta, G. (2017). Hypoglycemia: when to treat? Clinical Medicine Insights: Pediatrics, 11, 1179556517748913.
20. Kesmodel, U. S. (2018). Cross‐sectional studies–what are they good for? Acta obstetricia et gynecologica Scandinavica, 97(4), 388-393.
21. Khardori, R. (2022, Dec 19, 2022). Type 2 Diabetes Mellitus Treatment & Management. Medscape. Retrieved 29 Dec 2022 from https://emedicine.medscape.com/article/117853-treatment
22. Mayo Clinic. (2022, Dec. 07, 2022). Diabetes. Retrieved 30 Dec, 2022 from https://www.mayoclinic.org/diseases-conditions/diabetes/symptoms-causes/syc-20371444#:~:text=Diabetes%20mellitus%20refers%20to%20a,brain's%20main%20source%20of%20fuel.
23. McAdams, B. H., & Rizvi, A. A. (2016). An Overview of Insulin Pumps and Glucose Sensors for the Generalist. Journal of Clinical Medicine, 5(1), 5. https://doi.org/10.3390/jcm5010005
24. Miller, T. A., & Dimatteo, M. R. (2013). Importance of family/social support and impact on adherence to diabetic therapy. Diabetes, metabolic syndrome and obesity: targets and therapy, 6, 421-426. https://doi.org/10.2147/DMSO.S36368
25. Morales, J., & Schneider, D. (2014). Hypoglycemia. The American journal of medicine, 127(10 Suppl), S17-24. https://doi.org/10.1016/j.amjmed.2014.07.004
26. Muche, E. A., & Mekonen, B. T. (2020). Hypoglycemia prevention practice and its associated factors among diabetes patients at university teaching hospital in Ethiopia: Cross-sectional study. PloS one, 15(8), e0238094. https://doi.org/10.1371/journal.pone.0238094
27. Ortiz, M. R. (2017). Hypoglycemia in Diabetes. Nurs Clin North Am, 52(4), 565-574. https://doi.org/10.1016/j.cnur.2017.07.006
28. Polonsky, W. H., & Henry, R. R. (2016). Poor medication adherence in type 2 diabetes: recognizing the scope of the problem and its key contributors. Patient preference and adherence, 10, 1299-1307. https://doi.org/10.2147/PPA.S106821
29. Robert, A. A., & Al Dawish, M. A. (2020). The Worrying Trend of Diabetes Mellitus in Saudi Arabia: An Urgent Call to Action. Curr Diabetes Rev, 16(3), 204-210. https://doi.org/10.2174/1573399815666190531093735
30. Sancini, A., Ricci, S., Tomei, F., Sacco, C., Pacchiarotti, A., Nardone, N., . . . Tomei, G. (2017). Work related stress and blood glucose levels. Annali di Igiene – Medicina Preventiva e di Comunità, 29(2), 123-133. https://doi.org/10.7416/ai.2017.2139
31. Sarteau, A. C., Kahkoska, A. R., Crandell, J., Igudesman, D., Corbin, K. D., Kichler, J. C., . . . Mayer-Davis, E. (2023). More hypoglycemia not associated with increasing estimated adiposity in youth with type 1 diabetes. Pediatric Research, 93(3), 708-714. https://doi.org/10.1038/s41390-022-02129-1
32. Senior, P., & Hramiak, I. (2019). Fast-Acting Insulin Aspart and the Need for New Mealtime Insulin Analogues in Adults With Type 1 and Type 2 Diabetes: A Canadian Perspective. Canadian journal of diabetes, 43(7), 515-523. https://doi.org/10.1016/j.jcjd.2019.01.004
33. Shafiee, G., Mohajeri-Tehrani, M., Pajouhi, M., & Larijani, B. (2012). The importance of hypoglycemia in diabetic patients. J Diabetes Metab Disord, 11(1), 17. https://doi.org/10.1186/2251-6581-11-17
34. Sircar, M., Bhatia, A., & Munshi, M. (2016). Review of Hypoglycemia in the Older Adult: Clinical Implications and Management. Canadian journal of diabetes, 40(1), 66-72. https://doi.org/10.1016/j.jcjd.2015.10.004
35. Sun, C.-A. (2014). The experience and the meaning of hypoglycemia to Cambodian diabetes patients: A qualitative study conducted in Phnom Penh, Cambodia University of Oslo]. University of Oslo. https://www.duo.uio.no/handle/10852/41391
36. Torimoto, K., Okada, Y., Hajime, M., Tanaka, K., & Tanaka, Y. (2018). Risk Factors of Hypoglycemia in Patients with Type 2 Diabetes Mellitus: A Study Based on Continuous Glucose Monitoring. Diabetes Technol Ther, 20(9), 603-612. https://doi.org/10.1089/dia.2018.0017
37. World Health Organization. (2021). Diabetes. https://www.who.int/health-topics/diabetes#tab=tab_1
38. World Medical Association. (2018). World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. World Medical Association. Retrieved April 14, 2020, from https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/
Sara K. Aldekheel - BSN, MSN, Diabetes Educator at Diabetes Center, King Saud Hospital.
Unaizah
The researchers declare that no conflicts of interest exist for this research work
Mahmoud A. Shahin - BSN, MSN, PhD, Associate Professor of Medical-Surgical and Critical Care Nursing, Nursing Department, Prince Sultan Military College of Health Sciences; ResearcherID: HJH-8298-2023; Scopus Author ID: 57219535767.
Al Amal, Dhahran 34313
The researchers declare that no conflicts of interest exist for this research work
|
|
1. Figure 1. Sample size calculation using power analysis. | |
| Subject | ||
| Type | Исследовательские инструменты | |
View
(217KB)
|
Indexing metadata ▾ | |
|
|
2. Figure 2. Relationship between experienced hypoglycemia episodes among the participants and their gender (N=280) | |
| Subject | ||
| Type | Исследовательские инструменты | |
View
(126KB)
|
Indexing metadata ▾ | |
|
|
3. Figure 3. Experience of hypoglycemic episodes to participants’ educational level (N=280) | |
| Subject | ||
| Type | Исследовательские инструменты | |
View
(195KB)
|
Indexing metadata ▾ | |
Aldekheel S., Shahin M. Hypoglycemic episodes among type 1 diabetic patients in Unaizah, Saudi Arabia: causes, management, and associated factors. Diabetes mellitus. 2024;27(1):69-80. https://doi.org/10.14341/DM13112

 |
117036, Russian Federation
11, Dmitriya Ul’yanova street, Moscow








































